
Abstract
To assess prevalence and associated factors of depression, anxiety and suicidal ideas in populations from Russia, we conducted in rural and urban regions in Bashkortostan/Russia two population-based studies (Ural Eye and Medical Study (UEMS), performed from 2015 to 2017; Ural Very Old Study (UVOS), performed from 2017 to 2020) which included participants aged 40 + years and 85 + years, respectively. Depression was assessed using the questionnaire of the Center for Epidemiologic Studies Depression Scale Scoresheet, and anxiety was examined applying the State Trait Inventory Anxiety Test. Suicidal ideas were explored by the question whether suicide had previously been thought of or attempted (and if yes, for what reasons). In the statistical analysis we assessed the mean of the main outcome parameter (depression score and anxiety score) and searched for associations between these parameters and other parameters in univariable and multivariable regression analyses. In the UEMS with 5893 individuals (age: 59.0 ± 10.7 years; range 40–94 years), higher depression score and anxiety score were associated (multivariable analysis) with more marked hearing loss (beta: 0.07; P < 0.001, and beta: 0.07; P < 0.0012, respectively) and worse visual acuity (beta: 0.04; P = 0.02; and beta: 0.03; P = 0.03, resp.), in addition to female sex, Russian ethnicity, lower educational level, less alcohol consumption, weaker hand grip strength, less physical activity, and higher prevalence of dry eye disease. Attempted suicide was reported by 88 (1.5%; 95% CI 1.2, 1.8) participants. Having thought of suicide within the last 6 months was reported by 63 (1.1%) individuals. Out of 1491 UVOS participants (age: 88.2 ± 2.8 years; range 85–100 years) with a mean depression score of 20.0 ± 10.3 (median 18; range 0–58), 916 (61.4%; 95% CI 59.0, 63.9) fulfilled the definition of depression (depressions core ≥ 16). Higher depression score and higher anxiety score correlated (multivariable analysis) with higher hearing loss score (beta: 0.07; P = 0.02, and beta: 0.08; P = 0.009, resp.) and worse visual acuity (beta: 0.13; P < 0.001, and beta: 0.09; P = 0.007, resp.), in addition to female sex, urban region, less physical activity, less fruit intake, and lower cognitive function. Overall, 15 (1.0%; 95% CI 0.50, 1.50) individuals had attempted or thought of suicide. In conclusion, the findings suggest that besides female sex, lower level of education and lower cognitive function, it was sensory impairment, namely vision and hearing impairment, which belonged to the determinants of depression and anxiety in these populations from Russia.
Similar content being viewed by others


Introduction
The Global Burden of Diseases, Injuries, and Risk Factors Study 2019 revealed that depression and anxiety belong to the 25 most common causes of health-related burden worldwide1,2,3,4. Depression with a lifetime prevalence of 2% to 15% is one of the most important risk factors for substantial disability. Anxiety disorders are common and disabling conditions which predominantly start during childhood, adolescence, and early adulthood and which affect almost twice as many women as men5. They often concur with depression, alcohol and other substance-use disorders, and personality disorders. Suicide and self-harm are other major health and societal problems globally, with the highest impact in low-income and middle-income regions6. Rather than having a single cause, suicide and self-harm are the result of a complex interplay of several factors that occur throughout the life course, and vary by sex, age, ethnicity, and geography.
Prevalence and associations of depression and anxiety in the regions of Central Asia and Russia have relatively rarely been examined so far7,8,9,10,11,12. Averina and colleagues examined in a population-based study in Arkhangelsk, Russia, in the period 1999–2000 more than 4500 participants aged 18–90 years and found a higher prevalence of self-reported depression, anxiety and/or sleeping disorders in women (68.7%) than in men (32.3%)7. A higher prevalence of depression was correlated with smoking and alcohol consumption. Gurina and coworkers examined community-dwelling adults aged 65 + years in a suburb of St. Petersburg and reported that 25.9% of the younger group (age 65–74 years) and 42.5% of the older group (age ≥ 75 years) were at risk for depression8. Cook assessed individuals 35–69 years old and recruited in a population-based manner in Arkhangelsk and Novosibirsk in the study period from 2015 to 20189. The prevalence of depression was 10.7% in women and 5.4% in men, and the prevalence of anxiety was 10 6.2% in women and 3.0% in men. These previous investigations had limitations, such as being focused mostly on urban populations, with the recruitment of their participants not fully population-based, and/or addressing only the main disorders of depression and/or anxiety and not including many additional diseases and parameters into their study design. It holds true in particular for associations between depression/anxiety and hearing and vision impairment. We therefore examined in a population-based manner the prevalence of depression and anxiety and their associations with a whole array of other diseases and parameters in populations from Russia.
Methods
Ural eye and medical study (UEMS)
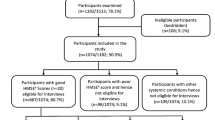
The UEMS is a population-based study which was performed in the Russian republic of Bashkortostan at the southwestern end of the Ural Mountains in the study period from 2015 to 201713,14. Study regions were the urban region of the Kirovskii district in Ufa as the capital of Bashkortostan and a rural region in the Karmaskalinsky District in a distance of 65 km from Ufa. The republic of Bashkortostan is situated between the Volga River and the Ural Mountains and is, with a population of 4 million people, the most populous republic in Russia. Inclusion criteria for the study were living in the study regions and an age of 40 + years. There were no exclusion criteria. Out of a total group of 7328 eligible individuals, 5899 (80.5%) individuals (3319 [56.3%] women) with a mean age of 59.0 ± 10.7 years (range 40–94 years) participated in the study. The demographics and general characteristics of the population of the UEMS have described in detail recently13,14.
Ural very old study (UVOS)
The UVOS is also a population-based study with the inclusion criteria of an age of 85 + years and living in the study regions. There were no exclusion criteria. The UVOS was conducted in the same study regions as the UEMS, i.e., the urban Kirovskii district in Ufa and the rural region Karmaskalinsky District. Due to the stricter inclusion criterion of a minimal age of 85 years, the size of both study regions included into the investigation was larger in the UVOS than in the UEMS. The UVOS was carried out in the period from 2017 to 202015. Out of 1882 eligible inhabitants aged 85 + years and living in the study regions, 1526 (81.1%) persons participated in the UVOS. The eligible individuals also included the inhabitants of all three private small retirement homes located in the urban study region. The characteristics and demographic parameters of the UVOS population have described in detail recently15. The study populations of the UEMS and UVOS did not differ significantly in the sex and age distribution from the Russian population as explored in the census carried out in 201016. Both studies, the UEMS and the UVOS, were performed by the same examination team applying the same techniques and using the same devices. The designs of both studies were similar or almost identical, except for the age-related inclusion criterion. The reason to choose an age of 40 + years as inclusion criterion for the UVOS was to examine the prevalence of major disorders and their associated factors in a middle-aged and elderly population. After finishing the recruitment for the UEMS, it was realized that in the UEMS, as in almost any other population-based study with such an age criterion for participation, the fraction of the very old group was relatively small. It was then decided to conduct a second study, now focusing on the very old population, and we set an inclusion criterion of an age of 85 + years.
Ethics
The Ethics Committee of the Academic Council of the Ufa Eye Research Institute approved the UEMS and the UVOS, and informed written consent was obtained from all participants. If individuals could not fully understand or appeared to be not fully informed about the meaning of the survey and the examination procedure applied in the study, family members or study personal repeatedly explained it to them in separate sessions until the participants were aware of the study. If the individuals were cognitively markedly impaired, informed consent was additionally obtained from family members. All the methods from both the studies were performed in accordance with relevant guidelines and regulation.
Methods
Using a bus, the study participants in both studies were brought from their homes to the Ufa Eye Institute where a team of about 20 trained medical doctors and technicians performed all examinations. The data were collected and stored in datafiles by a team of statisticians. Those UVOS participants being too immobile for the transport, were examined at their homes. The series of examinations started with a detailed interview consisting of more than 250 standardized questions on the socioeconomic background, diet, smoking, alcohol consumption, physical activity, quality of life and vision, history of any type of injuries and inter-personal violence, health assessment questions, medical history including known diagnosis and therapy of major disorders, symptoms of chronic diseases such as chronic obstructive pulmonary disease, asthma, kidney disease, orthopedic disorders, epilepsy and polyneuropathy, cognitive function and hearing loss (Table 1) (Supplementary Material)13,15. The level of education was differentiated into 8 grades, including “illiterate”, “passed the 5th class”, “passed the 8th class”, “passed the 10th class”, “passed the 12th class”, “specialized secondary education”, “graduation”, and “post-graduation”. The questions included in the interview were taken from standardized interviews published in the literature, such as the National Eye Institute Visual Functioning Questionnaire-25 (VFQ-25), the Questionnaire for Verifying Stroke-Free Status (QVSFS) from the American Heart Association, and the Michigan Neuropathy Screening Instrument13,15. Cognitive function was examined applying Folstein´s Mini-Mental State Examination (MMSE) with a maximal score of 30 points17. The examinations further included anthropometry, blood pressure measurement, handgrip dynamometry, spirometry, biochemical analysis of blood samples taken under fasting conditions, measurement of visual acuity based on automatic and subjective refractometry, and examination of prevalence and degree of a dry eye disease (Table 1). As described previously, dry eye disease was assessed by specific questions in the questionnaire and by additional ophthalmological examinations including Schirmer’s test18,19. The Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER statement guidelines) for collecting the data were applied20
Depression was assessed using the questionnaire of the Center for Epidemiologic Studies Depression Scale (CES-D) Scoresheet, and we examined anxiety using the State Trait Inventory Anxiety Test21,22,23,24. The participants of the UVOS could select one of four replies [“rarely or none of the time (less than one day)”/“some or a little of the time (1–2 days)”,/“occasionally or a moderate amount of time (3–4 days)”/“most or all of the time (5–7 days)”]. The participants of the UEMS had the choice between two replies (“some or a little of the time (1–2 days) or more rarely” versus “occasionally or a moderate amount of time (3–4 days) or more frequently”). Suicidal ideas were assessed by the question whether suicide had previously been attempted (and if yes, for what reasons including financial reasons), and whether one had thought of suicide and for what reasons.
Statistical analysis
Inclusion criteria for the present study were the availability of measurements of the depression score and anxiety score. Using a statistical software package (SPSS for Windows, version 27.0, IBM-SPSS, Chicago, IL, USA), we assessed the mean values and standard deviations main outcome parameters, i.e., the depression score and anxiety score and searched for associations between these parameters and other parameters, first in univariable linear regression analyses and followed by multivariable linear regression analyses. For that purpose, the values of categorical parameters with more than two possible values (e.g., “degree of processing meat (weak–medium–strong)”) were converted into points (i.e., weak—1, medium—2, strong—3). The multivariable regression analysis included the depression score or the anxiety score as dependent variable and as independent parameters all those variables which were associated with the depression score or the anxiety score in the univariable analysis with a P-value of ≤ 0.10. We chose a cut-off value of ≤ 0.10 to reduce the risk of missing a parameter the association of which might have become statistically significant in the eventual multivariable analysis. In a step-by-step manner, we first dropped parameters with collinearity (i.e., a variance inflation factor (VIF) of > 3), before we dropped those parameters out of the list of independent parameters that were no longer significantly associated with the depression score or anxiety score. We then added parameters, which previously dropped out, again to the model to test for the significance of their potential association with the depression and anxiety score. The prevalence of parameters such as depression was described as mean and its 95% confidence intervals (CIs). We calculated the standardized regression coefficient beta, the non-standardized regression coefficient B and its 95%CIs. All P-values were two-sided and were considered statistically significant when the values were less than 0.05.
Results
Ural eye and medical study (UEMS)
Out of the 5899 participants of the UEMS, the present investigation included 5893 (99.0%) individuals (3315 [56.3%] women) with measurements of the depression score and anxiety score. The mean age was 59.0 ± 10.7 years (median: 58 years; range 40–94 years). The group of study participants as compared with the group of individuals without measurement of the depression score and anxiety score did not differ significantly in age (P = 0.28) and sex (P = 0.61).
The mean depression score (theoretical maximum value: 20) was 5.2 ± 3.7 (median: 5; range 0–19), and the mean anxiety score (theoretical maximum value: 20) was 6.3 ± 3.5 (median: 6; range 0–20). Using a cut-off value of 6 or higher for the definition of depression, 2443/5893 (41.5%; 95% CI 40.2, 42.7) participants had depression.
In univariable analysis, a higher depression score was associated (P ≤ 0.1) with a multitude of parameters including age (beta: 0.12; B: 0.04; 95% CI 0.03, 0.05; P < 0.001) and sex (beta: 0.22; B: 1.67; 95% CI 1.49, 1.86; P < 0.001) (Table 1). In the multivariable regression analysis with the depressions core as dependent variable, we dropped various parameters due to collinearity or due to lack of statistical significance. In the final model, a higher depression score was associated with female sex, Russian ethnicity, lower level of education, higher prevalence of any alcohol consumption, lower number of days with fruit intake, lower self-reported salt consumption, higher prevalence of a history of angina pectoris, headache and thoracic spine pain, cardiovascular disease including stroke, skin diseases, thyroid gland disorders, falls and unconsciousness, lower dynamometric hand grip force, shorter duration of working day, lower prevalence of moderate physical activity in leisure time, lower number of days per week with walking or using a bicycle for at least 10 min to go to and from places, higher hearing loss score, worse best corrected visual acuity binocular or in the better eye, and higher prevalence of dry eye disease (Table 2). When we added the parameters of age (P = 0.99), region of habitation (P = 0.42), systolic blood pressure (P = 0.55), stage of arterial hypertension (P = 0.83), body height (P = 0.39), body mass index (P = 0.41), waist-hip circumference ratio (P = 0.24), waist-height ratio (P = 0.07), current smoking (P = 0.58), smoking package years (P = 0.14), self-reported salt intake (P = 0.06), and food containing whole grain (P = 0.90) as single parameters to the model, they were not significantly associated with the depression score.
A higher anxiety score correlated (multivariable analysis) with female sex, higher waist-hip circumference ratio, lower level of education, higher prevalence of any alcohol consumption, lower number of days with fruit intake, higher prevalence of a history of headache, thoracic spine pain and backache, cardiovascular disease including stroke, skin diseases, thyroid gland disorders, and unconsciousness, lower dynamometric hand grip force, lower prevalence of moderate physical activity in leisure time, higher prevalence of chronic obstructive pulmonary disease, higher hearing loss score, lower best corrected visual acuity, and higher prevalence of dry eye disease (Table 3). When we added the parameters of age (P = 0.15), region of habitation (P = 0.45), systolic blood pressure (P = 0.33), stage of arterial hypertension (P = 0.39), body mass index (P = 0.60), waist-height ratio (P = 0.12), current smoking (P = 0.94), smoking package years (P = 0.52), self-reported salt intake (P = 0.12), and food containing whole grain (P = 0.32) as single parameters to the model, they were not significantly associated with the depression score.
Out of the 5893 participants of the UEMS, 88 (1.5%; 95% CI 1.2, 1.8) reported to have attempted suicide, with 20 individuals out of the 88 indicating financial reasons for their attempt. Having thought of suicide was reported by 63 (1.1%) individuals, with 37 (0.6%) study participants stating, that they thought so within the last 6 months. Overall, 131 (2.2%; 95% CI 1.9, 2.6) individuals attempted or thought of suicide. A higher prevalence of having thought of or having attempted suicide correlated with younger age, lower level of education, lower number of days with fruit intake, higher prevalence of reported thoracic spine pain, unconsciousness and vigorous activity in leisure time, lower hand grip force, higher hearing loss score, and higher prevalence of dry eye disease (Table 4). When we replaced the parameter of hand grip force with the parameter of sex, female sex was associated with a higher prevalence of suicidal thoughts/attempts (OR 2.41; 95% CI 1.52, 3.80). When we added the parameters of region of habitation (P = 0.71), systolic blood pressure (P = 0.57), stage of arterial hypertension (P = 0.98), body mass index (P = 0.91), waist-hip ratio (P = 0.17), waist-height ratio (P = 0.97), current smoking (P = 0.64), smoking package years (P = 0.76), self-reported salt intake (P = 0.07), and food containing whole grain (P = 0.19) as single parameters to the model, they were not significantly associated with the prevalence of having thought of or having attempted suicide.
Ural very old study (UVOS)
Out of 1526 participants of the Ural Very Old Study, measurements of the depression score and anxiety score were available for 1491 (97.7%) individuals [382 (25.6%) men] with a mean age of 88.2 ± 2.8 years (range 85–100 years). The group of study participants as compared with the group of individuals without measurement of the depression and anxiety scores was significantly younger (88.2 ± 2.8 years versus 88.6 ± 3.1 years; P = 0.03), while both groups did not differ significantly in sex (P = 0.22).
The mean depression score (theoretical maximal value: 60) was 20.0 ± 10.3 (median: 18; range 0–58). Using a cut-off value of 16 or higher for the definition of depression, 916/1491 (61.4%; 95% CI 59.0, 63.9) participants had depression. A higher depression score was associated with female sex, urban region of habitation, lower number of days with fruit intake, lower prevalence of vigorous activity in leisure time, higher prevalence of a history of headache, higher hearing loss score, worse visual acuity, lower cognitive function, and lower prevalence of self-reported chronic obstructive pulmonary disease (Table 5). When we added the parameters of age (P = 0.78), systolic blood pressure (P = 0.40), stage of arterial hypertension (P = 0.23), body height (P = 0.051), body mass index (P = 0.73), waist-hip circumference ratio (P = 0.08), waist-height ratio (P = 0.62), current smoking (P = 0.32), self-reported salt intake (P = 0.92), number of cups of coffee taken daily (P = 0.86), number of cups of tea taken daily (P = 0.24), preference of black or green tea (P = 0.47), and food containing whole grain (P = 0.39) as single parameters to the model, they were not significantly associated with the depression score.
A higher anxiety score correlated with female sex, urban region of habitation, lower number of days with fruit intake, more time spent with sitting or reclining, less vigorous physical activity in leisure time, higher prevalence of a history of headache, higher hearing loss score, worse best corrected visual acuity, higher prevalence of chronic obstructive pulmonary disease, a lower cognitive function score (Table 6). When we added the parameters of age (P = 0.18), systolic blood pressure (P = 0.43), stage of arterial hypertension (P = 0.33), body mass index (P = 0.61), waist-hip circumference ratio (P = 0.15), waist-height ratio (P = 0.79), current smoking (P = 0.54), self-reported salt intake (P = 0.75), number of cups of coffee taken daily (P = 0.56), number of cups of tea taken daily (P = 0.95), preference of black or green tea (P = 0.70), and food containing whole grain (P = 0.57) as single parameters to the model, they were not significantly associated with the depression score.
Out of the 1491 participants of the UVOS, 14 (0.95%; 95% CI 0.45, 1.43) reported to have attempted suicide, with 3 individuals out of the 14 indicating financial reasons for their attempt. Other reasons were the daughter´s death (n = 1), feeling alone (n = 1). Having thought of suicide within the last 6 months was reported by 7 (0.5%; 95% CI 0.1, 0.8) study participants, and 10 (0.7%; 95% CI 0.3, 1.1) individuals overall declared to have thought of suicide. Overall, 15 (1.0%; 95% CI 0.50, 1.50) individuals attempted or thought of suicide. The overall number of participants having attempted or thought of suicide was too small for a meaningful detailed statistical analysis of associations.
Discussion
In the UVOS and in the UEMS, a higher depression score was associated with parameters such as female sex, urban region of habitation, lower physical activity, higher hearing loss score, worse visual acuity, and lower cognitive function. In the UVOS and in the UEMS, 15/1491 (1.0%) individuals and 131/5893 (2.2%) had attempted or thought of suicide. These findings agree with observations made in previous studies on other populations and ethnicities. Associations between a higher score of depression or anxiety with female sex, urban region of habitation, and lower physical activity have been found in previous investigations2,25. A correlation between depression and pain (in our study headache) have also been reported26. In a similar manner, the association between more physical activity and a lower score of depression as detected in our study is in agreement with previous investigations27,28. In our study, depression and anxiety score were not correlated with the prevalence of diabetes in the multivariable analysis. It mostly agrees with a recent meta-analysis in which it remained unclear whether and into which direction diabetes was related with depression29.
Of interest were the findings that a higher hearing loss score and a worse visual acuity were determinants of higher depression and anxiety, in the old population of the UVOS as well as in the middle-aged study population of the UEMS. It confirms previous studies, such as the investigation conducted by Kim and colleagues, in which the rate of depression was higher in a severe hearing-impaired group of patients as compared to a control group30,31,32,33,34,35,36. In the National Health and Aging Trends Study, a nationally representative survey in the USA, symptoms of depression and of anxiety were significantly more common in participants with self-reported vision impairment than in those individuals without self-reported vision impairment36. In a study from Britain on 13,900 individuals aged 75 + years, visually impaired individuals had a higher prevalence of depression compared with people with good vision. Of visually impaired older people, 13.5% were depressed, while anxiety was not markedly associated with vision impairment34.
These findings are paralleled by reports from Kuo and colleagues that the prevalence of hearing and vision impairment was associated with a decreased cognitive function, which was a determinant of a higher depression and anxiety scores in our study population37. In a similar manner, a longitudinal study of older US adults from the Health and Retirement Study found higher hazards of incident dementia for individuals with self-reported visual impairment, hearing impairment and dual sensory impairment as combination of both types of impairment compared to individuals without such impairments38,39,40.
Of interest may also be the associations between higher scores of depression or anxiety with a higher prevalence of dry eye disease. It agrees with observations made in previous epidemiologic studies18,41,42,43. In a national veterans population study, Galor and colleagues examined the association between DED and psychiatric disorders and found that depression was associated with a twofold increased risk of having DED18. Kim and associates reported in their population-based cross-sectional study a positive correlation between depression and dry eye symptoms41. In other smaller scaled case control investigations, the scores of depression and anxiety were associated with DED signs42.
From a practical point of view, the relationship between depression or anxiety with vision and hearing impairment and with dry eye disease may perhaps open possibilities for prevention and therapy, since all three conditions can be treated. Future studies may examine whether improvement of vision and hearing impairment may precent the development of depression and anxiety.
The relationship of a lower hand grip force strength with a higher score of depression/anxiety or of having thought of or having attempted suicide agrees with previous reports by Ashdown-Franks and others. It also agrees with general associations of a stronger hand grip force and lower all-cause death, lower cardiovascular death, and lower prevalence of cardiovascular disease44,45.
When the results of our studies are discussed, their limitations should be taken into account. First, in both studies, the UEMS and the UVOS, the primary participation rate was around 80%, so that non-participation might have led to a recruitment bias. In particular in the case of the UVOS, one may however take into account, that the high age of the UVOS participants with a minimum of 85 years was associated with a relatively high rate of immobility so that some individuals could not participate in the study. Second, the study area of both studies was typical for Southern Russia with respect to geography, climate and demography. With respect to ethnicity, Russians had a lower percentage in the study samples than in the populations in Central or North-Western Russia. Third, the cross-sectional design of our investigation did not allow to examine longitudinal cause-effect relationships so that we assessed factors associated with, but not risk factors of, the main outcome parameters. Fourth, the univariate analyses included a large list of variables, so that the statistical relevance of the single analysis would have had to be corrected for its dependence of performing a multitude of statistical comparisons. In the multivariable analysis however the inter-dependencies between the independent variables and the correction for the number of statistical tests performed was taken into account. Fifth, It may also be considered that the methods to assess depression and anxiety differ between previous investigations, so that differences in the results between the previous studies and the present investigation have to be discussed with respect to the differences in the techniques applied. Strengths of our project were that the outcome parameters of depression and anxiety have only rarely been examined in Russia, Eastern Europe and Central Asia, the relatively old age of the UVOS population, and the high number of disease and associations addressed in that both the UEMS and the UVOS.
In conclusion, besides female sex, lower level of education and lower cognitive function, it was sensory impairment, namely vision and hearing impairment, which belonged to the determinants of depression and anxiety.
Data availability
All identified data are available upon reasonable request from the corresponding author.
References
GBD 2019 Disease and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 396, 1204–1222 (2019).
Malhi, G. S. & Mann, J. J. Depression. Lancet 392, 2299–2312 (2018).
Alexopoulos, G. S. Depression in the elderly. Lancet 365, 1961–1970 (2005).
Moussavi, S. et al. Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet 370, 851–858 (2007).
Craske, M. G. & Stein, M. B. Anxiety. Lancet 388, 3048–3059 (2016).
Knipe, D., Padmanathan, P., Newton-Howes, G., Chan, L. F. & Kapur, N. Suicide and self-harm. Lancet 399, 1903–1916 (2022).
Averina, M. et al. Social and lifestyle determinants of depression, anxiety, sleeping disorders and self-evaluated quality of life in Russia: A population-based study in Arkhangelsk. Soc. Psychiatry Psychiatr. Epidemiol. 40, 511–518 (2005).
Gurina, N. A., Frolova, E. V. & Degryse, J. M. A roadmap of aging in Russia: The prevalence of frailty in community-dwelling older adults in the St Petersburg district: The “Crystal” study. J. Am. Geriatr. Soc. 59, 980–988 (2011).
Cook, S. et al. Prevalence of symptoms, ever having received a diagnosis and treatment of depression and anxiety, and associations with health service use amongst the general population in two Russian cities. BMC Psychiatry. 20, 537 (2020).
Dubinina, E. et al. Physical activity is associated with sleep quality: Results of the ESSE-RF Epidemiological Study. Front. Psychol. 12, 705212 (2021).
Shal’nova, S. A. et al. The prevalence of anxiety and depression in different regions of the Russian Federation and its association with sociodemographic factors (according to the data of the ESSE-RF study). Ter. Arkhiv 86, 53–60 (2014).
Maksimov, S. A. et al. Mental health of the Russian Federation population versus regional living conditions and individual income. Int. J. Environ. Res. Public Health 20, 5973 (2023).
Bikbov, M. M. et al. Prevalence of myopic maculopathy among adults in a Russian population. JAMA Netw. Open. 3, e200567 (2020).
Bikbov, M. M. et al. Frequency and associated factors of bone fractures in Russians: The Ural Eye and Medical Study. Sci. Rep. 8, 7483 (2018).
Bikbov, M. M. et al. Prevalence factors associated with vision impairment and blindness among individuals 85 years and older in Russia. JAMA Netw. Open. 4, e2121138 (2021).
Federal State Statistic Service. Population Census. https://eng.gks.ru/folder/76215. Accessed 5 Mar 2022.
Folstein, M. F., Folstein, S. E. & McHugh, P. R. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198 (1975).
Galor, A. et al. Prevalence and risk factors of dry eye syndrome in a United States veterans affairs population. Am. J. Ophthalmol. 152, 377–384 (2011).
Wolffsohn, J. S. et al. TFOS DEWS II diagnostic methodology report. Ocul. Surf. 15, 539–574 (2017).
Stevens, G. A. et al. Guidelines for accurate and transparent health estimates reporting: The GATHER statement. Lancet. 388, e19-23 (2016).
Lewinsohn, P. M., Seeley, J. R., Roberts, R. E. & Allen, N. B. Center for epidemiological studies-depression scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol. Aging. 12, 277–287 (1997).
Radloff, L. S. The CES-D scale: A self report depression scale for research in the general population. Appl. Psychol. Meas. 1, 385–401 (1977).
Thomas, J. L., Jones, G. N., Scarinci, I. C., Mehan, D. J. & Brantley, P. J. The utility of the CES-D as a depression screening measure among low-income women attending primary care clinics: The center for epidemiologic studies-depression. Int. J. Psychiatry Med. 31, 25–40 (2001).
Spielberger, C., Gorsuch, R. L. & Lushene, R. E. Manual for the State-Trait Anxiety Inventory (Consulting Psychologists Press, 1970).
Read, J. R., Sharpe, L., Modini, M. & Dear, B. F. Multimorbidity and depression: A systematic review and meta-analysis. J. Affect. Disord. 221, 36–46 (2017).
Bair, M. J., Robinson, R. L., Katon, W. & Kroenke, K. Depression and pain comorbidity: A literature review. Arch. Intern. Med. 163, 2433–2445 (2003).
Cooney, G. M. et al. Exercise for depression. Cochrane Database Syst. Rev. 9, 004366 (2013).
Kvam, S., Kleppe, C. L., Nordhus, I. H. & Hovland, A. Exercise as a treatment for depression: A meta-analysis. J. Affect. Disord. 202, 67–86 (2016).
Roy, T. & Lloyd, C. E. Epidemiology of depression and diabetes: A systematic review. J. Affect. Disord. 142(Suppl), S8-21 (2012).
Rovner, B. W., Zisselman, P. M. & Shmuely-Dulitzki, Y. Depression and disability in older people with impaired vision: A follow-up study. J. Am. Geriatr. Soc. 44, 181–184 (1996).
Wallhagen, M. I., Strawbridge, W. J., Shema, S. J., Kurata, J. & Kaplan, G. A. Comparative impact of hearing and vision impairment on subsequent functioning. J. Am. Geriatr. Soc. 49, 1086–1092 (2001).
Kim, S. Y. et al. Severe hearing impairment and risk of depression: A national cohort study. PLoS ONE 12, e0179973 (2017).
Rutherford, B. R., Brewster, K., Golub, J. S., Kim, A. H. & Roose, S. P. Sensation and psychiatry: Linking age-related hearing loss to late-life depression and cognitive decline. Am. J. Psychiatry. 175, 215–224 (2018).
Evans, J. R., Fletcher, A. E. & Wormald, R. P. Depression and anxiety in visually impaired older people. Ophthalmology. 114, 283–288 (2007).
Park, H. W., Lee, W. & Yoon, J. H. Gender-related effects of vision impairment characteristics on depression in Korea. Ophthalm. Epidemiol. 25, 105–112 (2018).
Frank, C. R., Xiang, X., Stagg, B. C. & Ehrlich, J. R. Longitudinal associations of self-reported vision impairment with symptoms of anxiety and depression among older adults in the United States. JAMA Ophthalmol. 137, 793–800 (2019).
Kuo, P. L. et al. Prevalence of concurrent functional vision and hearing impairment and association with dementia in community-dwelling Medicare beneficiaries. JAMA Netw. Open. 4, e211558 (2021).
Maharani, A., Dawes, P., Nazroo, J., Tampubolon, G. & Pendleton, N. Associations between self-reported sensory impairment and risk of cognitive decline and impairment in the health and retirement study cohort. J. Gerontol. B 75, 1230–1242 (2020).
Davies, H. R., Cadar, D., Herbert, A., Orrell, M. & Steptoe, A. Hearing impairment and incident dementia: Findings from the English longitudinal study of ageing. J. Am. Geriatr. Soc. 65, 2074–2081 (2017).
Yamada, Y. et al. Dual sensory impairment and cognitive decline: The results from the shelter study. J. Gerontol. A 71, 117–123 (2016).
Kim, K. W. et al. Association between depression and dry eye disease in an elderly population. Invest. Ophthalmol. Vis. Sci. 52, 7954–7958 (2011).
Li, M., Gong, L., Chapin, W. J. & Zhu, M. Assessment of vision-related quality of life in dry eye patients. Invest. Ophthalmol. Vis. Sci. 53, 5722–5727 (2012).
Labbé, A. et al. Dry eye disease, dry eye symptoms and depression: The Beijing Eye Study. Br. J. Ophthalmol. 97, 1399–1403 (2013).
Ashdown-Franks, G. et al. Handgrip strength and depression among 34,129 adults aged 50 years and older in six low- and middle-income countries. J. Affect. Disord. 243, 448–454 (2019).
Leong, D. P. et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet. 386, 266–273 (2015).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
M.M.B., G.M.K., J.B.J. contributed to the study conception and design. Material preparation, data collection and analysis were performed by all authors (M.M.B., T.R.G., G.M.K., E.M.I., S.P.J., R.M.Z., A.A.F., A.M.T., L.I.G., D.A.K., L.A.M., J.B.J.). The first draft of the manuscript was written by J.B.J., S.P.J. and M.M.B., and all authors (M.M.B., T.R.G., G.M.K., E.M.I., S.P.J., R.M.Z., A.A.F., A.M.T., L.I.G., D.A.K., L.A.M., J.B.J.) commented on previous versions of the manuscript. All authors (M.M.B., T.R.G., G.M.K., E.M.I., S.P.J., R.M.Z., A.A.F., A.M.T., L.I.G., D.A.K., L.A.M., J.B.J.) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bikbov, M.M., Gilmanshin, T.R., Kazakbaeva, G.M. et al. Prevalence of depression, anxiety and suicidal ideas and associated factors, in particular sensory impairments, in a population of Bashkortostan in Russia. Sci Rep 13, 17256 (2023). https://doi.org/10.1038/s41598-023-44561-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-44561-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
