
Abstract
Goal adjustment capacities (i.e., goal disengagement and goal reengagement) are core self-regulatory resources theorized to buffer psychological well-being during intractable life circumstances. However, research has yet to examine whether these capacities protect well-being for individuals who encounter uncontrollable losses in their ability to pursue important life goals due to the COVID-19 pandemic. Using a nationally-representative sample of U.S. adults aged 18–80 (n = 292), the present longitudinal study examined the extent to which goal disengagement and reengagement predicted levels and change in psychological well-being for individuals who differed in perceived control over their goals early in the pandemic. Results from multilevel growth models showed that goal reengagement, but not goal disengagement, capacities predicted higher levels of well-being during the pandemic (lower perceived stress, depressive symptoms; higher life satisfaction, meaning in life). Moderation models showed the benefits of goal reengagement for well-being were pronounced among individuals who perceived pandemic-induced declines in control over their goals. Findings inform theories of motivation and self-regulation and point to the adaptive value of goal reengagement capacities during uncontrollable life circumstances.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The onset of the COVID-19 pandemic constituted a major life stressor that threatened important life goals and elicited psychological distress (De France et al., 2021; Hagger et al., 2020; Misamer et al., 2021; Wang et al., 2020). This period was characterized by substantial, and in some cases insurmountable, obstacles to goal attainment across multiple life domains due to widespread office and school closures, job insecurity and layoffs, travel restrictions, physical distancing guidelines, and stay at home orders (Fisher et al., 2020; Shanahan et al., 2020). Theories of motivation and self-regulation have identified goal adjustment capacities as core self-regulatory resources that can buffer declines in psychological well-being for individuals confronted with uncontrollable life circumstances that can render previously valued goals unattainable (Barlow et al., 2020; Wrosch et al., 2003a, 2003b). For example, evidence shows goal adjustment capacities foster well-being among populations experiencing intractable circumstances, such as those diagnosed with cancer, experiencing physical disability, or caregiving for a family member with mental illness (Dunne et al., 2011; Mens & Scheier, 2016; Wrosch et al., 2011). However, little is known about the role of goal adjustment capacities as a form of adaptive self-regulation that may protect well-being in response to the widespread experience of lost opportunities and increased goal constraints inherent to the pandemic (Fisher et al., 2020).
The present study used longitudinal data from a national sample of U.S. adults to examine the relationship between goal adjustment capacities (i.e., goal disengagement and goal reengagement) and psychological well-being during the onset of the COVID-19 pandemic. This period provided a unique context to examine the role of goal adjustment capacities during a “natural experiment” that was marked by the common experience of increased goal constraints and blockages across multiple life domains (Fisher et al., 2020; Rutter, 2007; Shanahan et al., 2020). We thus examined whether goal disengagement and goal reengagement capacities were associated with 2-month levels and changes in central indicators of psychological well-being that included perceived stress, depressive symptoms, life satisfaction, and meaning in life.
Although the pandemic affected the entire U.S. population, there is likely to remain substantial heterogeneity in the extent to which individuals were confronted with insurmountable obstacles to goal attainment during this period (Nikolaidis et al., 2022; Prati & Mancini, 2021). Our study sought to account for this heterogeneity in pandemic experience by examining the role of perceived control over valued goals as a contextual variable that may moderate the association between goal adjustment capacities and well-being. Informed by theories of motivation and self-regulation, our premise was that goal adjustment capacities may become paramount in preserving well-being for those who perceived losses of control over valued goals (Heckhausen et al., 2019; Wrosch & Scheier, 2020; Wrosch et al., 2003a, 2003b).
Goal adjustment capacities and psychological well-being
Most people are strongly motivated to shape their lives by engaging with goals in central life domains (Heckhausen et al., 2019). Prominent theories of motivation posit that after committing to a valued goal, individuals actively pursue these objectives using goal engagement strategies that facilitate: investing time and effort, seeking help from others, and maintaining goal commitment in the face of obstacles and setbacks (Heckhausen & Schulz, 1995; Heckhausen et al., 2010, 2019; Wrosch & Scheier, 2020).Footnote 1 This ubiquitous motivation to actively pursue and protect goals stems in part from their central role in providing a sense of purpose and direction that drives adaptive behaviors and facilitates psychological well-being across the lifespan (Carver & Scheier, 2000; Heckhausen et al., 2010, 2019; Wrosch & Scheier, 2020).
However, some goals cannot be achieved regardless of how much time and effort are invested. The experience of unattainable goals is a common phenomenon due to the selection of unrealistic goals, age-related developmental losses, or negative life events that create insurmountable obstacles to goal attainment (Barlow et al., 2020; Brandtstädter & Renner, 1990; Wrosch et al., 2003a, 2003b). When severe goal constraints are encountered, adaptive self-regulation has been theorized to depend on goal adjustment capacities that enable individuals to abandon and replace previously important goals that can no longer be achieved (Wrosch et al., 2003a, 2003b). Goal adjustment capacities refer to trait-like individual differences in goal disengagement and goal reengagement (Wrosch et al., 2003a, 2003b; Wrosch & Scheier, 2020; see also Brandtstädter & Renner, 1990). Goal disengagement reflects individual differences in the tendency to withdraw commitment and effort from goals that have become unattainable. Goal reengagement reflects individual differences in the tendency to identify, commit to, and actively pursue meaningful new objectives when previously valued goals become obsolete or unattainable (Wrosch et al., 2003a, 2003b).
Increasing evidence shows both goal adjustment capacities are associated with central indicators of psychological well-being, although the benefits of goal disengagement may be unique to negative indicators (Barlow et al., 2020; Wrosch & Scheier, 2020). For example, early cross-sectional research by (Wrosch et al., 2003a, 2003b) showed that goal reengagement capacity exhibited adaptive associations with both positive (higher meaning in life) and negative indicators of well-being (less perceived stress and depressive symptoms). In contrast, goal disengagement capacity was inversely associated with negative indicators of well-being (perceived stress, depressive symptoms), but was not associated with a positive indicator of well-being (meaning in life). Similar results were observed in subsequent longitudinal studies that found that goal reengagement, but not disengagement, was strongly associated with higher life satisfaction (Haase et al., 2021; Herrmann et al., 2019; Thompson et al., 2013; Wrosch & Miller, 2009; Zhu et al., 2015). Results from these studies are in line with recent meta-analytic findings on goal adjustment capacities and well-being (Barlow et al., 2020). Across 31 samples, goal reengagement capacities were associated with positive (r = 0.25) and negative (r = − 0.17) indicators of psychological well-being. Goal disengagement was associated with negative (r = − 0.12), but not positive (r = 0.02), measures of well-being.Footnote 2
These findings suggest that goal adjustment capacities may play an important role in preserving psychological well-being during the COVID-19 pandemic due to the widespread experience of intractable life circumstances (Hagger et al., 2020). Goal disengagement and reengagement are theorized to buffer against declines in well-being for those encountering major life stressors, such as the onset of a pandemic, that sharply curtail opportunities for goal striving and attainment (Wrosch & Scheier, 2020). Under such intractable circumstances, goal disengagement is posited to support well-being by preventing an accumulation of failure experiences and distress; in turn, goal reengagement is theorized to promote well-being by facilitating an attentional shift towards new goals, reducing distress associated with goal failure, and fostering a sense of coherence and purpose (Barlow et al., 2020; Wrosch & Scheier, 2020). Goal adjustment capacities may thus protect well-being during the early stages of the pandemic characterized by lost opportunities and increased goal constraints (Fisher et al., 2020). However, research has yet to examine this issue, and little is known about whether goal adjustment capacities contribute to preserved well-being during the COVID-19 pandemic.
Goal adjustment capacities and psychological well-being in low control conditions
Goal adjustment capacities and intractable circumstances
Goal adjustment capacities have long been theorized to be most adaptive for individuals confronted with uncontrollable goal constraints (Wrosch & Scheier, 2020; Wrosch, et al., 2003a, 2003b). And yet it remains an open question whether the protective influence of goal adjustment capacities on well-being is pronounced for those who report (perceive) losses of control over their goals. As summarized below, previous research has sought to address this issue indirectly by inferring the presence of uncontrollable goal constraints from the experience of intractable life circumstances with the potential to restrict goal pursuit (e.g., cancer diagnosis, advanced old age, regional economic constraints, etc.; Jobin & Wrosch, 2016; Mens & Scheier, 2016; Tomasik et al., 2010; Wrosch & Sabiston, 2013).
For example, several studies have examined the role of goal adjustment capacities in preserving well-being for cancer patients and survivors who experience health-related stressors that may erode control over valued goals. One early study found that goal reengagement, but not goal disengagement, capacities predicted increases in positive affect for breast cancer survivors (Wrosch & Sabiston, 2013). Subsequent longitudinal research on cancer patients yielded a similar pattern of results, such that only goal reengagement prospectively predicted declines in depressive and anxiety symptoms (Zhu et al., 2015), as well as increases in life satisfaction and purpose in life (Mens & Scheier, 2016; Thompson et al., 2013). However, a different pattern emerged in a study of caregivers who experienced intractable circumstances in providing care for family members with mental illness (Wrosch et al., 2011). In this population experiencing chronically stressful conditions, goal reengagement was associated with increased caregiver burden and purpose in life, whereas goal disengagement was associated with decreased caregiver burden and increased purpose in life. Collectively, these findings provide some mixed evidence that goal adjustment capacities could benefit well-being for individuals with limited control.
Studies of older adults also provide indirect evidence for the role of goal adjustment capacities in preserving psychological well-being under low control circumstances. Lifespan theory and research has documented how old age commonly involves the experience of increasing developmental constraints and losses that can undermine perceived and actual control over valued goals (Baltes & Baltes, 1990; Heckhausen et al., 2010, 2019). Previous findings point to the potential benefits of both goal disengagement and goal reengagement in supporting late life well-being. For example, research in older populations showed that goal disengagement was associated with reduced levels of anxiety and also predicted reduced depressive symptoms over time (Arends et al., 2013; Dunne et al., 2011; Jobin & Wrosch, 2016). These studies also point to the benefits of goal reengagement in old age, such that goal reengagement was associated with reduced cross-sectional and longitudinal depressive symptoms (Arends et al., 2013; Dunne et al., 2011; Jobin & Wrosch, 2016). Similar results have been observed in populations experiencing severe economic constraints. For example, research by Tomasik et al. (2010) showed that strategies that support goal disengagement protected well-being in German regions with limited economic opportunities. These findings in populations experiencing intractable life circumstances collectively imply that goal adjustment capacities may protect well-being when individuals lose control over important goals. However, research has yet to systematically test this central theoretical premise using a direct indicator of control over goals (Barlow et al., 2020; Wrosch & Scheier, 2020).
Goal adjustment capacities and low perceived control
Although the inference-based approaches used in past studies have contributed to our understanding of goal adjustment capacities, such methods come with limitations. This is because there is likely substantial heterogeneity in perceived and actual control over goals among individuals facing intractable circumstances (Chipperfield et al., 2017; Lachman et al., 2011; Perry et al., 2005; Thompson, 1999). In other words, there may be considerable variance in the degree to which people feel in (and have) controlFootnote 3 when they experience major life stressors that can threaten their goals such as a cancer diagnosis, economic constraints, age-related losses, or the COVID-19 pandemic. Our study thus sought to extend prior research by directly testing how participants’ self-reported (perceived) control over their goals may moderate the relationship between goal adjustment tendencies and psychological well-being during the pandemic.
Perceived control over goals refers to beliefs people hold about their capacity to influence valued goals and objectives in their lives (Chipperfield et al., 2017; Hamm, Heckhausen, et al., 2019; Robinson & Lachman, 2016). We focused on perceived control as moderator variable because it reflects a central motivational resource that supports psychological well-being by facilitating the achievement of goals across multiple domains and throughout the lifespan (Chipperfield et al., 2018; Drewelies et al., 2018; Infurna et al., 2011; Perry, 2003; Shane et al., 2012; Vargas Lascano et al., 2015). Decades of laboratory and field studies have shown that individuals with low perceived control or who report losses of control over their goals are at elevated risk of goal failure and vulnerable to declines in well-being (Abramson et al., 1980; Chipperfield et al., 2017; Lachman, 2006). This implies that goal adjustment capacities could become paramount in preserving well-being for individuals who perceive losses of control over valued goals.
Despite the fact that such control appraisals are posited to influence (moderate) the relationship between goal adjustment capacities and well-being, research has yet to directly test this theoretical proposition (Wrosch et al., 2003a, 2003b). Theories of motivation and self-regulation suggest that individuals who perceive they have lost control over valued goals need to disengage from the goal and to reengage with new goals in order to protect well-being and facilitate adaptive development (Heckhausen et al., 2010; Wrosch & Scheier, 2020). Noteworthy is that such a pronounced relationship between goal adjustment capacities and well-being for individuals with low perceived control may hold even under circumstances where individuals have high veridical (actual) control. This is because a perceived lack of control in such circumstances should still ultimately curtail motivated behavior and undermine well-being in the absence of goal adjustment (cf., Abramson et al., 1980; Weiner, 2018). In other words, theory and evidence suggest the perception that one has low control over a situation or goal erodes motivation, reduces goal striving, and threatens well-being even in circumstances when one has objective control (Abramson et al., 1980; Garber & Seligman, 1980; Lachman et al., 2011; Langer, 1975; Perry et al., 2005; Skinner, 1996; Thompson, 1999). In line with theoretical propositions (Wrosch & Scheier, 2020; Wrosch et al., 2003a, 2003b), this implies that strong goal adjustment capacities may be needed to maintain well-being for individuals who perceive losses of control over important goals.
Goal adjustment capacities and low perceived control during COVID-19
The pandemic provides a unique window of opportunity to examine the role of goal adjustment capacities in a low control environment considering that several features distinguish it from other intractable life circumstances. First, the pandemic engendered a unique set of contextual circumstances that may make some goals temporarily, but not permanently, obsolete. The pandemic thus has the potential to create “frozen” goals (Davydenko et al., 2019) that cannot currently be pursued due to severe constraints but that can potentially be reactivated in the future once circumstances change. Second, the pandemic can be conceptualized as a global “natural experiment” in that it affected everyone (Rutter, 2007). The pandemic had the capacity to create severe goal blockages in multiple domains and for adults across the lifespan due to widespread office and school closures, job insecurity and layoffs, travel restrictions, physical distancing guidelines, and stay at home orders (Fisher et al., 2020; Shanahan et al., 2020).
Third, despite the nature of this “natural experiment” that affected everyone to some extent, there is likely to remain substantial heterogeneity in the degree to which the pandemic created insurmountable obstacles to goal attainment (Fisher et al., 2020; Pearman et al., 2020). For example, heterogeneity in perceived control has been observed despite the widespread experience of increased constraints and lost opportunities during the pandemic (Fisher et al., 2020; Pearman et al., 2020). Thus, although many individuals may perceive declines in control over important goals during this period, others may experience stability or even increases in control. Adaptive self-regulation for those who experience pandemic-related losses of control over valued goals may depend on their capacity to disengage from unattainable goals and reengage with alternative goals (Heckhausen et al., 2019; Wrosch & Scheier, 2020). We sought to shed light on this issue by examining whether the benefits of goal adjustment capacities for well-being were pronounced for individuals who perceived pandemic-related losses of control over their goals.
The present study
Our study examined the extent to which goal adjustment capacities predicted 2-month levels and changes in psychological well-being during the first wave of the COVID-19 pandemic. We focused on central indicators of well-being that have been linked to goal adjustment capacities and shown to be affected by the pandemic: perceived stress, depressive symptoms, life satisfaction, and meaning in life (Barlow et al., 2020; De France et al., 2021; Magson et al., 2021; Shanahan et al., 2020). Given their adaptive value under intractable life circumstances, we reasoned that goal adjustment capacities may facilitate well-being in response to the common experience of reduced opportunities and increased constraints inherent in the early stages of the pandemic (Arends et al., 2013; Fisher et al., 2020; Mens & Scheier, 2016; Wrosch et al., 2011). Specifically, informed by theories of self-regulation (Wrosch & Scheier, 2020), we expected that goal reengagement would predict levels and changes in each indicator of well-being, whereas goal disengagement would predict levels and changes in only the negative indicators of well-being (perceived stress, depressive symptoms). These differential hypotheses were based on recent meta-analytic findings showing that goal reengagement capacities were associated with both positive and negative indicators of well-being in a range of intractable circumstances, whereas goal disengagement capacities were associated only with negative indicators (Barlow et al., 2020).
We also expected that individual differences in perceived control would moderate the associations between goal adjustment capacities and psychological well-being. Informed by theory (Barlow et al., 2020; Wrosch & Scheier, 2020), our premise was that the protective influence of goal adjustment capacities should become paramount for individuals who experienced pandemic-induced declines in control over their goals. We expected the association between goal reengagement and levels and changes in each indicator of well-being to be strongest for individuals who reported reduced perceptions of control over their goals. We also expected the association between goal disengagement and levels and changes in the negative indicators of well-being (perceived stress, depressive symptoms) to be pronounced for individuals with reduced control. Goal reengagement and goal disengagement were expected to have lesser benefits for individuals who may not need to adjust their goals due to stability or even increased perceived control over their goals.
Method
Participants and procedure
We examined our research questions using data from the NDSU National COVID Study. This ongoing study was conducted with a representative sample of 301 U.S. adults aged 18–80 who were recruited via Prolific.co during the early stages of the COVID-19 pandemic. We planned to recruit 300 participants to maximize sample size with available funds while obtaining three-waves of data on a sample that was nationally representative for age, sex, and race. Participants were compensated for their time at all waves. Demographic, psychosocial, and health data were collected online via a secure survey platform over three waves. The first wave of data collection occurred in mid-April (April 16) during the peak of the first wave of the COVID-19 pandemic in the U.S. The second and third waves occurred 2 weeks (May 1) and 2 months (June 17) after the first wave.
Because we were interested in examining whether goal adjustment capacities predicted levels and changes in psychological well-being over time, study inclusion criteria were that participants provided data at two or more waves (Hamm et al., 2021; Wrosch et al., 2018). Participants in the analyzed sample (n = 292) had a mean age of 45 years (range 18–80), were 50% female, were racially diverse (71% White, 14% Black, 8% Asian, 4% two or more races, 3% other), had an average household income of $53,486 (range 0–200,000), and had completed 16 years of education on average (range 12–24). Based on results of a recent simulation study (Arend & Schäfer, 2019), our sample of 292 individuals with 3 waves of data provided adequate power (> 80%) to detect small to medium effects of our Level 2 predictors on the intercepts and slopes of our outcome measures. We included six attention checks to ensure data quality were high. Responses to these items indicated participants in the analyzed sample were attentive (pass rate on each item exceeded 98%). Informed consent was obtained from all participants prior to participation, and the North Dakota State University Institutional Review Board approved all procedures and methods.
Measures
Goal adjustment capacities
Goal adjustment capacities were assessed at each wave using the 10-item Goal Adjustment Scale (Wrosch et al., 2003a, 2003b). The scale measures individual differences in peoples’ tendencies to disengage from unattainable goals (goal disengagement) and to reengage with new alternative goals (goal reengagement). Participants were asked to indicate how they usually reacted to situations where they were forced to stop pursuing important goals using 5-point scales (1 = strongly disagree, 5 = strongly agree). Four items assessed goal disengagement (e.g., “It’s easy for me to reduce my effort towards the goal”), and six items assessed goal reengagement (e.g., “I seek other meaningful goals”). Mean scores for each scale were computed for each wave. Goal disengagement (αs = 0.76–0.82) and goal reengagement (αs = 0.91–0.92) exhibited acceptable reliability within each wave and stability across waves (rs = 0.54–0.68, all ps < 0.01). Goal disengagement and goal reengagement were not strongly correlated (rs = 0.16–0.19) in line with recent meta-analytic findings (Barlow et al., 2020). Consistent with previous research (Wrosch et al., 2013), we averaged scores across waves to obtain individual difference measures of goal disengagement (M = 2.72, SD = 0.72) and goal reengagement capacities (M = 3.51, SD = 0.72). See Table 1 for a summary of descriptive statistics and intercorrelations between the study variables.
Perceived control
Perceived control over personal goals was measured at each wave by asking participants to rate how much control they currently had over their goals relative to before the pandemic. Participants responded to the item “Would you rate the amount of control you have over your personal goals as much less, a little bit less, about the same, a little bit more, or much more compared to before the coronavirus (COVID-19) outbreak?” on a 5-point scale (1 = much less control, 5 = much more control). Perceived control was positively correlated across waves (rs = 0.48-0.53, all ps < 0.01). Consistent with previous research (Hamm et al., 2021; Wrosch et al., 2018), we averaged scores across waves to obtain an individual difference measure of perceived control (M = 2.86, SD = 0.90).
Perceived stress
Perceived stress was assessed at each wave using the Perceived Stress Scale (Cohen et al., 1983). Participants rated how frequently they experienced 10 different situations over the past week (e.g., “How often have you been upset because of something that happened unexpectedly?”). Responses were recorded using a 5-point scale (1 = never, 5 = very often), and a mean score was computed for each wave. Perceived stress exhibited acceptable reliability at each wave (αs = 0.91–0.92). Average levels of perceived stress in our national sample (M = 2.63) were roughly half a standard deviation higher than mean average levels observed prior to the pandemic in other national U.S. samples (M = 2.19; Knight et al., 2021).
Depressive symptoms
The 10-item Center for Epidemiologic Studies Depression (CES-D10) scale was used to assess depressive symptoms at each wave (Björgvinsson et al., 2013; Radloff, 1977). Participants rated how frequently they had experienced each of 10 depressive symptoms during the past week using a four-point scale (1 = less than one day, 4 = 5–7 days). A mean depressive symptoms score was computed for each wave. The CES-D10 scale exhibited acceptable reliability at each wave (all αs = 0.89). Average levels of depressive symptoms in our national sample (M = 2.02) were slightly higher than mean average levels observed prior to the pandemic in other national U.S. samples (M = 1.82; Haner et al., 2019).
Life satisfaction
The Satisfaction with Life Scale (SWLS) was used to measure life satisfaction at each wave (Diener et al., 1985). Participants rated their agreement with five items that assessed how satisfied they were with their current life circumstances (e.g., “I am satisfied with my life”). Responses were recorded using a 7-point scale (1 = strongly disagree, 7 = strongly agree), and a mean score was computed for each wave. Life satisfaction exhibited acceptable reliability at each wave (αs = 0.93–0.94). Average levels of life satisfaction in our national sample (M = 3.84) were roughly half a standard deviation lower than mean average levels observed prior to the pandemic in other national U.S. samples (Ms = 4.29, 4.95; Anderson et al., 2012; Chen & Feeley, 2014).
Meaning in life
The PROMIS Meaning and Purpose scale was used to measure meaning in life at each wave (Salsman et al., 2014). Participants rated their agreement with six items that included, for example, “I have a good sense of what makes my life meaningful”, “I experience deep fulfillment in my life”, and ‘My life has purpose.” Responses were recorded using a 5-point scale (1 = strongly disagree, 5 = strongly agree) and a mean score was computed for each wave. Meaning in life exhibited acceptable reliability at each wave (αs = 0.93–0.94).
Demographic covariates
Baseline age, sex, income, and education were included as covariates in the analyses. Age in years (M = 44.99, SD = 16.23) and sex (1 = male, 2 = female; 50% female) were based on self-reports. Participants reported their total household income in US dollars (M = 53,483, SD = 39,505) and the number of years of formal education they had completed (M = 16.27, SD = 2.37).
Results
Rationale for analyses
Multilevel growth model analyses were conducted in a stepwise fashion. Step 1 involved preliminary (descriptive) growth models to identify average levels of, and changes in, each indicator of psychological well-being during the first wave of the pandemic. Step 2 involved main effect growth models that examined whether goal disengagement and goal reengagement capacities predicted levels and changes in well-being. Step 3 involved interaction effect growth models that tested whether associations between goal disengagement, goal reengagement, and levels and changes in well-being were moderated by perceived control. Predictive models in Steps 2–3 controlled for baseline differences in age, sex, education, and income. All models were estimated with Mplus 8 (Muthén & Muthén, 1998–2017), with missing data handled using full-information maximum likelihood estimation.
Step 1: 2-month levels and changes in well-being (preliminary growth models)
Prior to conducting preliminary (descriptive) multilevel growth models, we assessed empty multilevel models to determine intraclass correlations (ICCs) for our outcome variables. ICCs exceeded 0.80 for all indicators of psychological well-being: perceived stress (0.83), depressive symptoms (0.85), life satisfaction (0.90), and meaning in life (0.84). These ICCs indicated that a large majority (over 80%) of the variance in our outcome measures over the 2-month study period was due to between-person differences.
Preliminary multilevel growth models were subsequently estimated to identify 2-month levels and changes in well-being during the first wave of the pandemic. We estimated two-level models with measurement occasions (Level-1) nested within participants (Level-2). Level-1 models included an intercept, person-centered score of time in study, and a residual term. We person-centered time in all models based on recommendations by Blozis and Cho (2008) who showed that non-centered time can result in underestimating the random slope coefficients. The intercepts in these models represented average levels of (individual differences in) well-being across the 2-month study. Time slopes in these models represented the amount of monthly change in each indicator of well-being. Level-2 models included random effects for the intercept and time slope.
Intercepts in these models indicated that, on average, participants in the present study reported levels of perceived stress (2.63), depressive symptoms (2.02), life satisfaction (3.84), and meaning in life (3.62) that approached the midpoint of each scale. Considerable variance was observed for these Level-1 intercepts (\(\tau_{u0}^{2}\) range = 0.477–2.704, SEs = 0.042–0.231, ps < 0.001). Time slopes in these models showed that, on average, perceived stress (γ = − 0.06, SE = 0.014, p < 0.001) and depressive symptoms declined over the 2-month study period (γ = − 0.05, SE = 0.011, p < 0.001). Life satisfaction remained relatively stable (γ = 0.03, SE = 0.023, p = 0.251), whereas meaning in life decreased (γ = − 0.04, SE = 0.016, p = 0.019). Relatively limited variability around the Level-1 time slopes were observed in these models: perceived stress (\(\tau_{u1}^{2}\) = 0.016, SE = 0.007, p = 0.026), depressive symptoms (\(\tau_{u1}^{2}\) = 0.007, SE = 0.004, p = 0.123), life satisfaction (\(\tau_{u1}^{2}\) = 0.046, SE = 0.012, p < 0.001), and meaning in life (\(\tau_{u1}^{2}\) = 0.014, SE = 0.007, p = 0.029).
Step 2: Predicting 2-month levels and changes in well-being (main effect models)
Multilevel growth models were estimated to test whether goal disengagement and goal reengagement capacities predicted levels and 2-month changes in psychological well-being. We estimated two-level models with measurement occasions (Level-1) nested within participants (Level-2). Level-1 models included an intercept, person-centered score of time in study, and a residual term. Level-1 models were specified as follows:
Level-2 covariates included baseline age, sex, income, and education, as well as individual differences in perceived control (PC), goal disengagement (GD), and goal reengagement (GR). All Level-2 predictors were grand-mean centered. Level-2 models were specified as follows:
Results showed that goal reengagement capacities were associated with lower levels of perceived stress and depressive symptoms and higher levels of life satisfaction and meaning in life over the study period (see Table 2). Goal reengagement also predicted 2-month declines in perceived stress, but was not associated with changes in depressive symptoms, meaning, or life satisfaction. Goal disengagement capacities did not predict levels or change in the outcome measures, with the exception that they were associated with lower levels of meaning. Perceived control was associated with more adaptive levels of each indicator of well-being, but did not predict changes in well-being over time.
Step 3: Predicting 2-month levels and changes in well-being (interaction effect models)
Multilevel growth models were estimated to test whether perceived control over personal goals moderated the relationships between goal disengagement, goal reengagement, and levels and changes in well-being. Level-1 and Level-2 models were specified as shown in Step 2. The only difference was that Level-2 models included Goal Disengagement (GD) x Perceived Control (PC) and Goal Reengagement (GR) × Perceived Control (PC) interaction terms. All Level-2 predictors were grand-mean centered. Level-2 models were specified as follows:
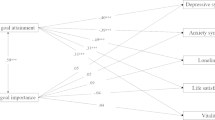
A consistent pattern of Goal Reengagement x Perceived Control interactions emerged for levels of, but not changes in, each indicator of well-being (see Table 3). Simple slope analyses probed the interactions and assessed the effects of goal reengagement at low (− 1 SD) and high (+ 1 SD) levels of perceived control (Cohen et al., 2002; Hayes, 2018). As expected, results indicated the benefits of goal reengagement were strongest for individuals who reported low control over their goals (see Figs. 1, 2). For those with low control, goal reengagement predicted lower levels of perceived stress (γ = − 0.49, SE = 0.086, p < 0.001) and depressive symptoms (γ = − 0.45, SE = 0.075, p < 0.001) and higher life satisfaction (γ = 1.04, SE = 0.183, p < 0.001) and meaning in life (γ = 0.84, SE = 0.095, p < 0.001). For those with high control, goal reengagement remained beneficial, but the magnitudes of the associations were reduced by over half for all outcomes: perceived stress (γ = − 0.11, SE = 0.081, p = 0.163), depressive symptoms (γ = − 0.14, SE = 0.071, p = 0.054), life satisfaction (γ = − 0.34, SE = 0.172, p = 0.046), and meaning in life (γ = 0.34, SE = 0.090, p < 0.001). Goal Disengagement x Perceived Control interactions were not significant for levels or changes in the outcome measures.

Goal reengagement × perceived control interactions predicting average levels of perceived stress and depressive symptoms over the 2-month study period. Simple slopes of goal reengagement with 95% confidence intervals are presented at low (− 1 SD) and high (+ 1 SD) levels of perceived control

Goal reengagement × perceived control interactions predicting average levels of life satisfaction and meaning in life over the two-month study period. Simple slopes of goal reengagement with 95% confidence intervals are presented at low (− 1 SD) and high (+ 1 SD) levels of perceived control
We also probed the Goal Reengagement x Perceived Control interactions by examining the effects of perceived control at low (− 1 SD) and high (+ 1 SD) levels of goal reengagement capacity. Simple slope analyses showed that, for those with low goal reengagement, perceived control was a strong predictor of perceived stress (γ = − 0.41, SE = 0.075, p < 0.001), depressive symptoms (γ = − 0.34, SE = 0.065, p < 0.001), and life satisfaction (γ = 0.65, SE = 0.159, p < 0.001), and meaning in life (γ = 0.45, SE = 0.083, p < 0.001). For those with high goal reengagement, perceived control effects were reduced to non-significance for all outcomes (ps = 0.081–0.499). As shown in Figs. 1 and 2, this suggests that experiencing losses of control over valued goals was associated with poor well-being for only individuals with limited goal reengagement capacities. In other words, goal reengagement buffered the otherwise detrimental consequences of low control on psychological well-being.Footnote 4
Supplemental analyses
Baseline predictors
Our main analyses were based on mean-averaged measures of goal disengagement, goal reengagement, and perceived control to capture individual differences in the predictor variables across the study period. Supplemental multilevel models tested whether results were consistent when predictor variables were based on only the wave 1 (baseline) assessment. Results were in line with those observed in the main analyses. Main effect models showed that goal reengagement predicted more adaptive levels of each indicator of well-being (γs =|0.18–0.46|, ps < 0.001), as well as marginally steeper declines in perceived stress over time (γ = − 0.03, p = 0.081). Interaction effect models showed that the Goal Reengagement x Perceived Control interaction term remained a significant predictor of levels of all well-being indicators (γs =|0.09–0.22|, ps = 0.001–0.026).
Supplemental measure of perceived control
Our main analyses were based on a single-item measure of perceived control that captured intraindividual comparisons of how much control participants perceived they currently had over their goals relative to before the pandemic. Multilevel models were conducted to evaluate whether results were consistent when using a supplemental two-item measure of perceived control that incorporated a distinct, but related, measure of current control over goals that did not involve an intraindividual comparison to pre-pandemic levels of control.Footnote 5 Results were in line with those observed in the main analyses. Main effect models showed that goal reengagement predicted more adaptive levels of each indicator of well-being (γs =|0.25–0.60|, ps < 0.001), as well as steeper declines in perceived stress over time (γ = − 0.05, p = 0.023). Interaction effect models showed that, with the exception of depressive symptoms (γ = 0.08, p = 0.105), the Goal Reengagement x Perceived Control interaction term remained a significant predictor of levels of perceived stress (γ = 0.14, p = 0.007), life satisfaction (γ = − 0.22, p = 0.047), and meaning in life (γ = − 0.16, p = 0.007).
Separate models
Our main analyses assessed the unique influence of goal disengagement and goal reengagement on psychological well-being by simultaneously including both goal adjustment capacities as predictor variables in each model. Supplemental multilevel models tested whether results remained unchanged when goal disengagement and goal reengagement were analyzed in separate models that did not control for the other goal adjustment capacity. Results were consistent with those observed in the main analyses. Main effect models showed that only goal reengagement predicted more adaptive levels of each indicator of well-being (γs =|0.28–0.69|, ps < 0.001), as well as steeper declines in perceived stress over time (γ = − 0.05, p = 0.026). Interaction effect models showed that only the Goal Reengagement × Perceived Control interaction terms remained significant predictors of levels of the well-being indicators (γs =|0.18–0.40|, ps < 0.001–0.005).
Discussion
Using longitudinal data from a nationally-representative sample of American adults, our study sought to shed light on the role of goal adjustment capacities during the first wave of the COVID-19 pandemic. Findings advance the literature in providing initial evidence that goal reengagement, but not goal disengagement, may facilitate well-being in response to the intractable circumstances inherent in the early stages of pandemic. Results also inform theories of motivation and self-regulation in showing that goal reengagement may become paramount for individuals who perceive losses of control over valued goals (Heckhausen et al., 2019; Wrosch & Scheier, 2020).
Goal adjustment capacities and psychological well-being during COVID-19
Participants in our national sample reported levels of perceived stress, depressive symptoms, life satisfaction, and meaning in life that were near the scale midpoints. We observed modest changes over time in these indicators of well-being with limited variability in the average trajectories. The modest change and limited variability may be due in part to the relatively brief 2-month period over which the study occurred. Specifically, perceived stress, depressive symptoms, and meaning in life slightly declined on average, whereas life satisfaction was fairly stable. Results are largely in line with past longitudinal research which found slight declines or relative stability in perceived stress and depressive symptoms (Kujawa et al., 2020; Wang et al., 2020; Yarrington et al., 2021) and relatively stability in life satisfaction (Aknin et al., 2022; Hartstone & Medvedev, 2021; Li et al., 2021) during the early stages of the pandemic. Stability in life satisfaction could be due in part to (downward) social comparison processes that may have led individuals to believe their lives could have been substantially worse than they were given the circumstances (cf. Aknin et al., 2022). Less is known about trajectories of meaning in life over the course of the pandemic, and it is interesting that it declined on average in contrast to the stability observed for life satisfaction. We speculate that meaning may have exhibited slight declines during this initial stage of the pandemic as people adjusted to reduced opportunities to engage in social and work activities that provide important sources of meaning. However, we note that while the 2-month decline in meaning was significant in our sample, the rate of decline was relatively modest (less than 1/10 of an SD).
The present longitudinal study is unique in examining the implications of individual differences in goal adjustment capacities for psychological well-being during the COVID-19 pandemic. Findings point to the importance of goal reengagement in supporting adaptive levels of well-being under intractable life circumstances. Strong goal reengagement capacities predicted maintaining higher levels of well-being across all indicators over the 2-month study period, which may be due to the capacity of goal reengagement to redirect effort towards new activities shown to support well-being during the pandemic (e.g., exercising, hobbies; Fullana et al., 2020; Lades et al., 2020). Results are in line with theory and extend previous research showing that the capacity to reengage with new goals is associated with preserved well-being across the adult lifespan (Barlow et al., 2020; Haase et al., 2021; Mens & Scheier, 2016; Wrosch & Scheier, 2020; Wrosch, et al., 2003a, 2003b).
As expected, goal reengagement also predicted adaptive changes (faster declines) in perceived stress over time. However, we did not observe goal reengagement effects on the time slopes of the other indicators of well-being. This may be due in part to the relative stability over time in the well-being indicators that characterized our sample. In other words, the non-significant goal reengagement effects on change over time in these indicators may be partly a function of the limited within-person variance (high ICCs) and limited variance in the time slopes of these well-being outcomes (Hoffman, 2015; Snijders & Bosker, 2011).
Goal disengagement capacities were unrelated to levels of, or changes in, our outcome measures, with the exception that it was associated with lower levels of meaning in life. This was contrary to our expectation that goal disengagement would predict adaptive levels and changes in the negative indicators of well-being, as observed in previous research (although see Neter et al., 2009; O’Connor et al., 2009 for exceptions). These findings may be due in part to the relatively brief timeframe over which our study data were collected. Goal disengagement capacities are thought to facilitate well-being by preventing emotional distress from repeated failure experiences that typically accumulate over more extended timeframes in response to goals that have become permanently unattainable (Wrosch, et al., 2003a, 2003b). Our findings point to the possibility that goal disengagement capacities could be less beneficial over shorter time intervals during junctures when goals may become temporarily “frozen” (e.g., during the onset of the pandemic). The adaptive value of goal disengagement may have become apparent with a longer follow-up period in response to goals that were permanently lost.
The adaptive value of goal adjustment capacities when experiencing losses of control over valued goals
Our study was the first to examine the role of perceived control in moderating the relationship between goal adjustment capacities and psychological well-being. Findings extend previous research (Wrosch & Scheier, 2020) by showing that goal adjustment capacities may be paramount for individuals who perceive pandemic-related losses of control over important goals. In particular, a consistent pattern was observed across outcomes such that high goal reengagement, but not goal disengagement, was associated with greater levels of well-being for those with reduced perceptions of control over their goals due to the pandemic.Footnote 6
Theory and evidence suggest that individuals with low perceived control are at elevated risk of goal failure and vulnerable to declines in well-being (Chipperfield et al., 2017; Lachman, 2006; Robinson & Lachman, 2016). Our findings were consistent with this argument in showing individuals who experienced pandemic-induced declines in control over valued goals reported significantly higher perceived stress, more depressive symptoms, lower life satisfaction, and less meaning in life (see Table 2). Goal adjustment capacities may be particularly adaptive under such low control circumstances to the extent they foster disengagement from unattainable goals and reengagement with alternate goals that can alleviate distress and provide a new sense of meaning and purpose.
Our results were largely in line with this logic in showing that goal reengagement had pronounced benefits for well-being among those who lost control over their goals. The pattern of predicted values for those who reported reductions in control, but who varied in their levels of goal reengagement is particularly noteworthy (see Figs. 1, 2). Across indicators, we observed the lowest levels of well-being for those with reduced control over their goals who also reported their capacity for goal reengagement was limited. In contrast, we observed substantially higher, and relatively normal, levels of well-being for those with reduced control who had strong goal reengagement capacities. In other words, those who lost control over their goals but reported high goal reengagement experienced similar levels of perceived stress, depressive symptoms, life satisfaction, and meaning in life during the pandemic as their peers who experienced stability or even increases in their control over valued goals. This suggest that goal reengagement buffered against the negative consequences for well-being that were otherwise observed for individuals who reported pandemic-related declines in control over their goals. The strong influence of goal reengagement in this population whose goal pursuits were severely curtailed by the pandemic may have been due to its capacity to redirect effort towards meaningful new activities (Fullana et al., 2020; Lades et al., 2020). In doing so, goal reengagement could have reduced distress associated with failed goals, and provided a new source of meaning and satisfaction in daily life. As expected, goal reengagement had lesser benefits for those who reported increased perceived control over their goals who presumably had little need to adjust their goals given their continued capacity to influence and achieve these objectives.
We observed no moderated associations between goal disengagement capacities and levels or changes in the indicators of psychological well-being. As noted in relation to the absence of goal disengagement main effects, this may potentially be due to the relatively brief follow-up period during a juncture when goals may have become temporarily “frozen” rather than permanently lost. Goal disengagement capacities may have exhibited a more beneficial pattern of associations with well-being over a longer time interval to the extent that disengaging from truly obsolete goals prevents an accumulation of failures and distress (Wrosch, et al., 2003a, 2003b).
Strengths, limitations, and future directions
Our study has several strengths. First, it was informed by strong theories of motivation and self-regulation that address individual differences in goal adjustment capacities and perceived control (Heckhausen et al., 2010, 2019; Lachman, 2006; Wrosch & Scheier, 2020; Wrosch et al., 2003a, 2003b). The fundamental principles of these theoretical frameworks are clear, specific, testable, and supported by over 15 years of empirical evidence. Second, our sample was drawn from a nationally-representative sample of U.S. adults aged 18–80, thus enhancing the generalizability of study findings. Third, the present findings were based on longitudinal data from three assessments that occurred over a 2-month period during the first peak of the pandemic. Our data thus enabled a unique examination of the consequences of goal adjustment on levels and changes in our outcome measures during a period of heightened uncertainty and unpredictability.
Although using longitudinal data from the NDSU National COVID Study is a strength, it also represents a limitation to the extent that data on goal-specific disengagement and reengagement were not assessed. Consistent with previous research, we used the well-established goal adjustment scale to capture domain-general goal adjustment (Wrosch et al., 2003a, 2003b). Future research is needed to consider how goal-specific disengagement and reengagement may buffer against losses in well-being for individuals who lose control over important goals. A second limitation is the use of a single-item measure to assess perceived control over goals. However, we note that this measure exhibited acceptable test–retest reliability across waves (rs = 0.48–0.53), and, as reported in the supplemental analyses, results were consistent when using a two-item measure of perceived control that included a distinct, but related, measure of goal-specific control (which did not involve a comparison to pre-pandemic levels of goal control). A third potential limitation is that our data collection occurred online. However, we took precautions to ensure data quality were high by including six attention checks (pass rate on each item exceeded 98%) and retaining only participants who responded to at least two waves in the analyzed sample. Another limitation concerns the relatively limited variance observed for change in our outcome measures (the time slopes). Further research that spans longer periods of time is needed to test whether the association between goal adjustment capacities and changes over time in well-being may be moderated by perceived control. Although our use of a national U.S. sample is a strength of the present study, it is unclear whether findings may generalize to other countries. Future research is needed to examine generalizability across nations with different cultures and pandemic responses.
The present study points to several avenues for future research. For example, although the unique combination of characteristics (global natural experiment, heterogeneity in goal blockages, frozen goals) that define the pandemic distinguishes it from other life circumstances, we note that each characteristic does not apply exclusively to the pandemic. Research is needed to examine the role of goal adjustment capacities in other circumstances that share some of these characteristics and have the potential to indefinitely render many goals unattainable (e.g., natural disasters, civil war, or death of a spouse/divorce). Research in this vein would contribute to a more nuanced understanding of the broader set of life circumstances in which goal disengagement and/or goal reengagement capacities may become paramount. Such studies would also contribute to scientific knowledge of boundary conditions for the benefits of goal disengagement and goal reengagement.
Research is also needed to examine the role of goal adjustment capacities in fostering positive health behaviors and outcomes during the COVID-19 pandemic and other major life stressors. Previous research has shown that goal disengagement and goal reengagement are linked to adaptive health behaviors, such as increased sleep efficiency and physical activity in breast cancer survivors (Castonguay et al., 2017; Mens & Scheier, 2016). However, little is known about the extent to which goal adjustment capacities can buffer declines in positive health behaviors for normative populations who encounter goal blockages due to the pandemic. Future research is also needed to document the behavioral mechanisms, such as adaptive health behaviors (e.g., exercise) and hobbies (e.g., cooking, crafting), that may link goal adjustment capacities to well-being. Further research is also needed to examine whether the associations between goal adjustment capacities and well-being are reciprocal in nature. Results of our study taken together with recent evidence that certain facets of well-being can predict goal reengagement point to this possibility (Haase et al., 2021).
Our findings suggest another productive area for future research may be the development of motivational and self-regulatory interventions designed to increase goal reengagement capacities in populations who perceive losses of control over valued goals. There is increasing evidence that conceptually-related motivation interventions to increase goal engagement can facilitate well-being, goal striving, and achievement for populations who experience (surmountable) setbacks and obstacles during goal pursuit (Gitlin et al., 2006; Hamm et al., 2016; Hamm, Heckhausen, et al., 2019; Hamm, Perry, et al., 2019). Interventions to foster goal reengagement may be particularly adaptive for populations who encounter severe goal constraints and losses of control. However, previous research suggests the potential importance of also targeting increases in goal disengagement capacities for populations who are faced with goals that have become permanently obsolete (Barlow et al., 2020; Wrosch & Scheier, 2020). Research is thus needed to evaluate the potential of interventions to facilitate goal disengagement and/or goal reengagement capacities for those who encounter insurmountable constraints and uncontrollable life circumstances that render previously important goals unattainable.
Data availability
Study data are available from the authors on request.
Notes
-
We note several important conceptual distinctions between goal adjustment capacities (goal disengagement and goal reengagement) as discussed and operationalized by Wrosch et al. (2003a, 2003b, 2020) relative to compensatory secondary control (goal disengagement) as discussed by Heckhausen et al. (2010, 2019). Foremost among these differences is that Wrosch et al.’s conceptualization concerns individual differences in trait-like tendencies to disengage from unattainable goals and to reengage with new attainable goals (after encountering an unattainable goal). In contrast, Heckhausen et al. focus on how individuals seek to actively shape their lives using control strategies that operate in service of goal engagement or disengagement and facilitate adaptive responses to goal-relevant obstacles and setbacks.
-
It is important to note that while goal disengagement may be adaptive in the long term, giving up on valued goals is often experienced as unpleasant. Instances of goal disengagement may thus be associated with short-term decreases, followed by long-term increases, in psychological well-being (Barlow et al., 2020; Körner et al., 2012; Tomasik & Salmela-Aro, 2012; Tomasik & Silbereisen, 2012).
-
We note that both perceived and actual (veridical) control over goals are important with respect to psychological well-being. Perceived and actual control are presumed to be intricately connected in adulthood with the line separating the two blurred in real-world field studies (cf. Heckhausen & Schulz, 1995; Lachman & Weaver, 1998; Perry et al., 2005; Skinner, 1996). However, it would be very difficult to assess actual (true) declines in control over goals in a field study such as our own. Doing so would rely on inferring losses of control based on the presence of intractable life circumstances that have the potential to restrict goal pursuit (e.g., job loss, cancer diagnosis, physical disability, etc.). As discussed above, this approach is limited to the extent that there is likely substantial heterogeneity in actual control over goals among individuals facing intractable circumstances (e.g., control over career goals among individuals who lost their job).
-
Supplemental multilevel models tested whether there was a three-way Goal Disengagement x Goal Reengagement x Perceived Control interaction for each outcome. The three-way interaction did not predict levels or changes in the study outcome measures (ps > .30).
-
These were the only two measures of control over goals assessed in the present study.
-
As discussed above, the absence of moderated goal reengagement effects on change over time may be a function of the limited within-person variance (high ICCs) and limited variance in the time slopes of these well-being outcomes.
References
Abramson, L. Y., Garber, J., & Seligman, M. E. P. (1980). Learned helplessness in humans: An attributional analysis. Human Helplessness: Theory and Applications, 3, 34.
Aknin, L. B., Neve, J.-E.D., Dunn, E. W., Fancourt, D. E., Goldberg, E., Helliwell, J. F., Jones, S. P., Karam, E., Layard, R., Lyubomirsky, S., Rzepa, A., Saxena, S., Thornton, E. M., VanderWeele, T. J., Whillans, A. V., Zaki, J., Karadag, O., & Amor, Y. B. (2022). Mental health during the first year of the COVID-19 pandemic: A review and recommendations for moving forward. Perspectives on Psychological Science. https://doi.org/10.1177/17456916211029964
Anderson, C., Kraus, M. W., Galinsky, A. D., & Keltner, D. (2012). The local-ladder effect: Social status and subjective well-being. Psychological Science, 23(7), 764–771. https://doi.org/10.1177/0956797611434537
Arend, M. G., & Schäfer, T. (2019). Statistical power in two-level models: A tutorial based on Monte Carlo simulation. Psychological Methods, 24(1), 1–19. https://doi.org/10.1037/met0000195
Arends, R. Y., Bode, C., Taal, E., & Van de Laar, M. A. F. J. (2013). The role of goal management for successful adaptation to arthritis. Patient Education and Counseling, 93(1), 130–138. https://doi.org/10.1016/j.pec.2013.04.022
Baltes, P. B., & Baltes, M. M. (1990). Psychological perspectives on successful aging: The model of selective optimization with compensation. In P. Baltes & M. M. Baltes (Eds.), Successful aging: Perspectives from the behavioral sciences (pp. 1–34). Cambridge University Press.
Barlow, M. A., Wrosch, C., & McGrath, J. J. (2020). Goal adjustment capacities and quality of life: A meta-analytic review. Journal of Personality, 88(2), 307–323. https://doi.org/10.1111/jopy.12492
Björgvinsson, T., Kertz, S. J., Bigda-Peyton, J. S., McCoy, K. L., & Aderka, I. M. (2013). Psychometric properties of the CES-D-10 in a psychiatric sample. Assessment, 20(4), 429–436.
Blozis, S. A., & Cho, Y. I. (2008). Coding and centering of time in latent curve models in the presence of interindividual time heterogeneity. Structural Equation Modeling: A Multidisciplinary Journal, 15(3), 413–433.
Brandtstädter, J., & Renner, G. (1990). Tenacious goal pursuit and flexible goal adjustment: Explication and age-related analysis of assimilative and accommodative strategies of coping. Psychology and Aging, 5(1), 58.
Carver, C. S., & Scheier, M. F. (2000). On the structure of behavioral self-regulation. In M. Boekaerts, M. Zeidner, & P. R. Pintrich (Eds.), Handbook of self-regulation (pp. 41–84). Elsevier.
Castonguay, A. L., Wrosch, C., & Sabiston, C. M. (2017). The roles of negative affect and goal adjustment capacities in breast cancer survivors: Associations with physical activity and diurnal cortisol secretion. Health Psychology, 36(4), 320–331. https://doi.org/10.1037/hea0000477
Chen, Y., & Feeley, T. H. (2014). Social support, social strain, loneliness, and well-being among older adults: An analysis of the Health and Retirement Study. Journal of Social and Personal Relationships, 31(2), 141–161. https://doi.org/10.1177/0265407513488728
Chipperfield, J. G., Hamm, J. M., Perry, R. P., & Ruthig, J. C. (2017). Perspectives on studying perceived control in the twenty-first century. In M. D. Robinson & M. Eid (Eds.), The happy mind: Cognitive contributions to well-being (pp. 215–233). New York: Springer.
Chipperfield, J. G., Perry, R. P., Pekrun, R., Hamm, J. M., & Lang, F. R. (2018). Paradoxical effects of perceived control on survival. The Journals of Gerontology: Series B, 73(7), 1166–1174. https://doi.org/10.1093/geronb/gbx002
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385. https://doi.org/10.2307/2136404
Davydenko, M., Werner, K. M., & Milyavskaya, M. (2019). Frozen goals: Identifying and defining a new type of goal. Collabra Psychology, 5(1), 17. https://doi.org/10.1525/collabra.194
De France, K., Hancock, G. R., Stack, D. M., Serbin, L. A., & Hollenstein, T. (2021). The mental health implications of COVID-19 for adolescents: Follow-up of a four-wave longitudinal study during the pandemic. American Psychologist. https://doi.org/10.1037/amp0000838
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49(1), 71–75. https://doi.org/10.1207/s15327752jpa4901_13
Drewelies, J., Schade, H., Hülür, G., Hoppmann, C. A., Ram, N., & Gerstorf, D. (2018). The more we are in control, the merrier? Partner perceived control and negative affect in the daily lives of older couples. The Journals of Gerontology: Series B. https://doi.org/10.1093/geronb/gby009
Dunne, E., Wrosch, C., & Miller, G. E. (2011). Goal disengagement, functional disability, and depressive symptoms in old age. Health Psychology, 30(6), 763–770. https://doi.org/10.1037/a0024019
Fisher, J. R. W., Tran, T. D., Hammarberg, K., Sastry, J., Nguyen, H., Rowe, H., Popplestone, S., Stocker, R., Stubber, C., & Kirkman, M. (2020). Mental health of people in Australia in the first month of COVID -19 restrictions: A national survey. Medical Journal of Australia, 213(10), 458–464. https://doi.org/10.5694/mja2.50831
Fullana, M. A., Hidalgo-Mazzei, D., Vieta, E., & Radua, J. (2020). Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. Journal of Affective Disorders, 275, 80–81. https://doi.org/10.1016/j.jad.2020.06.027
Garber, J., & Seligman, M. E. (1980). Human helplessness: Theory and applications. Academic Press.
Gitlin, L. N., Winter, L., Dennis, M. P., Corcoran, M., Schinfeld, S., & Hauck, W. W. (2006). A randomized trial of a multicomponent home intervention to reduce functional difficulties in older adults: Multicomponent home intervention to reduce functional difficulties. Journal of the American Geriatrics Society, 54(5), 809–816. https://doi.org/10.1111/j.1532-5415.2006.00703.x
Haase, C. M., Singer, T., Silbereisen, R. K., Heckhausen, J., & Wrosch, C. (2021). Well-being as a resource for goal reengagement: Evidence from two longitudinal studies. Motivation Science, 7(1), 21–31. https://doi.org/10.1037/mot0000199
Hagger, M. S., Keech, J. J., & Hamilton, K. (2020). Managing stress during the coronavirus disease 2019 pandemic and beyond: Reappraisal and mindset approaches. Stress and Health. https://doi.org/10.1002/smi.2969
Hamm, J. M., Heckhausen, J., Shane, J., Infurna, F. J., & Lachman, M. E. (2019). Engagement with six major life domains during the transition to retirement: Stability and change for better or worse. Psychology and Aging, 34(3), 441–456. https://doi.org/10.1037/pag0000343
Hamm, J. M., Perry, R. P., Chipperfield, J. G., Heckhausen, J., & Parker, P. C. (2016). A motivation-enhancing treatment to sustain goal engagement during life course transitions. Motivation and Emotion, 40(6), 814–829. https://doi.org/10.1007/s11031-016-9576-4
Hamm, J. M., Perry, R. P., Chipperfield, J. G., Parker, P. C., & Heckhausen, J. (2019). A motivation treatment to enhance goal engagement in online learning environments: Assisting failure-prone college students with low optimism. Motivation Science, 5(2), 116–134. https://doi.org/10.1037/mot0000107
Hamm, J. M., Wrosch, C., Barlow, M. A., & Kunzmann, U. (2021). A tale of two emotions: The diverging salience and health consequences of calmness and excitement in old age. Psychology and Aging, 36(5), 626.
Haner, M., Sloan, M. M., Cullen, F. T., Kulig, T. C., & Lero Jonson, C. (2019). Public concern about terrorism: Fear, worry, and support for anti-Muslim policies. Socius. https://doi.org/10.1177/2378023119856825
Hartstone, J. M., & Medvedev, O. N. (2021). The role of mindfulness and life satisfaction in psychological distress during the COVID-19 Lockdown in New Zealand: A Quasi-experimental Study. Mindfulness. https://doi.org/10.1007/s12671-021-01731-4
Heckhausen, J., & Schulz, R. (1995). A life-span theory of control. Psychological Review, 102(2), 284.
Heckhausen, J., Wrosch, C., & Schulz, R. (2010). A motivational theory of life-span development. Psychological Review, 117(1), 32–60.
Heckhausen, J., Wrosch, C., & Schulz, R. (2019). Agency and motivation in adulthood and old age. Annual Review of Psychology, 70(1), 191–217. https://doi.org/10.1146/annurev-psych-010418-103043
Herrmann, M., Brandstätter, V., & Wrosch, C. (2019). Downgrading goal-relevant resources in action crises: The moderating role of goal reengagement capacities and effects on well-being. Motivation and Emotion, 43(4), 535–553. https://doi.org/10.1007/s11031-019-09755-z
Hoffman, L. (2015). Longitudinal analysis: Modeling within-person fluctuation and change. Routledge.
Infurna, F. J., Gerstorf, D., Ram, N., Schupp, J., & Wagner, G. G. (2011). Long-term antecedents and outcomes of perceived control. Psychology and Aging, 26(3), 559–575. https://doi.org/10.1037/a0022890
Jobin, J., & Wrosch, C. (2016). Goal disengagement capacities and severity of disease across older adulthood: The sample case of the common cold. International Journal of Behavioral Development, 40(2), 137–144. https://doi.org/10.1177/0165025415597549
Knight, E. L., Jiang, Y., Rodriguez-Stanley, J., Almeida, D. M., Engeland, C. G., & Zilioli, S. (2021). Perceived stress is linked to heightened biomarkers of inflammation via diurnal cortisol in a national sample of adults. Brain, Behavior, and Immunity, 93, 206–213. https://doi.org/10.1016/j.bbi.2021.01.015
Körner, A., Reitzle, M., & Silbereisen, R. K. (2012). Work-related demands and life satisfaction: The effects of engagement and disengagement among employed and long-term unemployed people. Journal of Vocational Behavior, 80(1), 187–196. https://doi.org/10.1016/j.jvb.2011.05.004
Kujawa, A., Green, H., Compas, B. E., Dickey, L., & Pegg, S. (2020). Exposure to COVID-19 pandemic stress: Associations with depression and anxiety in emerging adults in the United States. Depression and Anxiety, 37(12), 1280–1288. https://doi.org/10.1002/da.23109
Lachman, M. E. (2006). Perceived control over aging-related declines: Adaptive beliefs and behaviors. Current Directions in Psychological Science, 15(6), 282–286. https://doi.org/10.1111/j.1467-8721.2006.00453.x
Lachman, M. E., Neupert, S. D., & Agrigoroaei, S. (2011). The relevance of control beliefs for health and aging. In M. Boekaerts, M. Zeidner, & P. R. Pintrich (Eds.), Handbook of the psychology of aging (pp. 175–190). Elsevier.
Lades, L. K., Laffan, K., Daly, M., & Delaney, L. (2020). Daily emotional well-being during the COVID-19 pandemic. British Journal of Health Psychology, 25(4), 902–911. https://doi.org/10.1111/bjhp.12450
Langer, E. J. (1975). The illusion of control. Journal of Personality and Social Psychology, 32(2), 311–328. https://doi.org/10.1037/0022-3514.32.2.311
Li, Y., Luan, S., Li, Y., & Hertwig, R. (2021). Changing emotions in the COVID-19 pandemic: A four-wave longitudinal study in the United States and China. Social Science & Medicine, 285, 114222. https://doi.org/10.1016/j.socscimed.2021.114222
Magson, N. R., Freeman, J. Y. A., Rapee, R. M., Richardson, C. E., Oar, E. L., & Fardouly, J. (2021). Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. Journal of Youth and Adolescence, 50(1), 44–57. https://doi.org/10.1007/s10964-020-01332-9
Mens, M. G., & Scheier, M. F. (2016). The benefits of goal adjustment capacities for well-being among women with breast cancer: Potential mechanisms of action: Goal adjustment, well-being, and breast cancer. Journal of Personality, 84(6), 777–788. https://doi.org/10.1111/jopy.12217
Misamer, M., Signerski-Krieger, J., Bartels, C., & Belz, M. (2021). Internal locus of control and sense of coherence decrease during the COVID-19 pandemic: A survey of students and professionals in social work. Frontiers in Sociology, 6, 174. https://doi.org/10.3389/fsoc.2021.705809
Neter, E., Litvak, A., & Miller, A. (2009). Goal disengagement and goal re-engagement among multiple sclerosis patients: Relationship to well-being and illness representation. Psychology & Health, 24(2), 175–186. https://doi.org/10.1080/08870440701668665
Nikolaidis, A., DeRosa, J., Kass, M., Droney, I., Alexander, L., Di Martino, A., Bromet, E., Merikangas, K., Milham, M. P., & Paksarian, D. (2022). Heterogeneity in COVID-19 pandemic-induced lifestyle stressors predicts future mental health in adults and children in the US and UK. Journal of Psychiatric Research, 147, 291–300. https://doi.org/10.1016/j.jpsychires.2021.12.058
O’Connor, R. C., Fraser, L., Whyte, M.-C., MacHale, S., & Masterton, G. (2009). Self-regulation of unattainable goals in suicide attempters: The relationship between goal disengagement, goal reengagement and suicidal ideation. Behaviour Research and Therapy, 47(2), 164–169. https://doi.org/10.1016/j.brat.2008.11.001
Pearman, A., Hughes, M. L., Smith, E. L., & Neupert, S. D. (2020). Mental health challenges of United States healthcare professionals during COVID-19. Frontiers in Psychology, 11, 2065. https://doi.org/10.3389/fpsyg.2020.02065
Perry, R. P. (2003). Perceived (academic) control and causal thinking in achievement settings. Canadian Psychology/psychologie Canadienne, 44(4), 312–331. https://doi.org/10.1037/h0086956
Perry, R. P., Hall, N. C., & Ruthig, J. C. (2005). Perceived (academic) control and scholastic attainment in higher education. In L. W. Perna & M. B. Paulsen (Eds.), Higher education: Handbook of theory and research (Vol. 20, pp. 363–436). Springer.
Prati, G., & Mancini, A. D. (2021). The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychological Medicine, 51(2), 201–211. https://doi.org/10.1017/S0033291721000015
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. https://doi.org/10.1177/014662167700100306
Robinson, S. A., & Lachman, M. E. (2016). Perceived control and behavior change: A personalized approach. Oxford University Press.
Rutter, M. (2007). Proceeding from observed correlation to causal inference: The use of natural experiments. Perspectives on Psychological Science, 2(4), 377–395. https://doi.org/10.1111/j.1745-6916.2007.00050.x
Salsman, J. M., Lai, J.-S., Hendrie, H. C., Butt, Z., Zill, N., Pilkonis, P. A., Peterson, C., Stoney, C. M., Brouwers, P., & Cella, D. (2014). Assessing psychological well-being: Self-report instruments for the NIH Toolbox. Quality of Life Research, 23(1), 205–215. https://doi.org/10.1007/s11136-013-0452-3
Shanahan, L., Steinhoff, A., Bechtiger, L., Murray, A. L., Nivette, A., Hepp, U., Ribeaud, D., & Eisner, M. (2020). Emotional distress in young adults during the COVID-19 pandemic: Evidence of risk and resilience from a longitudinal cohort study. Psychological Medicine. https://doi.org/10.1017/S003329172000241X
Shane, J., Heckhausen, J., Lessard, J., Chen, C., & Greenberger, E. (2012). Career-related goal pursuit among post-high school youth: Relations between personal control beliefs and control strivings. Motivation and Emotion, 36(2), 159–169. https://doi.org/10.1007/s11031-011-9245-6
Skinner, E. A. (1996). A guide to constructs of control. Journal of Personality and Social Psychology, 71(3), 549.
Snijders, T. A., & Bosker, R. J. (2011). Multilevel analysis: An introduction to basic and advanced multilevel modeling. Sage.
Thompson, E., Stanton, A. L., & Bower, J. E. (2013). Situational and dispositional goal adjustment in the context of metastatic cancer: Goal adjustment and metastatic cancer. Journal of Personality, 81(5), 441–451. https://doi.org/10.1111/jopy.12025
Thompson, S. C. (1999). Illusions of control: How we overestimate our personal influence. Current Directions in Psychological Science, 8(6), 187–190. https://doi.org/10.1111/1467-8721.00044
Tomasik, M. J., & Salmela-Aro, K. (2012). Knowing when to let go at the entrance to university: Beneficial effects of compensatory secondary control after failure. Motivation and Emotion, 36(2), 170–179. https://doi.org/10.1007/s11031-011-9246-5
Tomasik, M. J., & Silbereisen, R. K. (2012). Beneficial effects of disengagement from futile struggles with occupational planning: A contextualist-motivational approach. Developmental Psychology, 48(6), 1785–1796. https://doi.org/10.1037/a0026952
Tomasik, M. J., Silbereisen, R. K., & Heckhausen, J. (2010). Is it adaptive to disengage from demands of social change? Adjustment to developmental barriers in opportunity-deprived regions. Motivation and Emotion, 34(4), 384–398. https://doi.org/10.1007/s11031-010-9177-6
Vargas Lascano, D. I., Galambos, N. L., Krahn, H. J., & Lachman, M. E. (2015). Growth in perceived control across 25 years from the late teens to midlife: The role of personal and parents’ education. Developmental Psychology, 51(1), 124–135. https://doi.org/10.1037/a0038433
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., McIntyre, R. S., Choo, F. N., Tran, B., Ho, R., Sharma, V. K., & Ho, C. (2020). A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain, Behavior, and Immunity, 87, 40–48. https://doi.org/10.1016/j.bbi.2020.04.028
Weiner, B. (2018). The legacy of an attribution approach to motivation and emotion: A no-crisis zone. Motivation Science, 4(1), 4–14. https://doi.org/10.1037/mot0000082
Wrosch, C., Amir, E., & Miller, G. E. (2011). Goal adjustment capacities, coping, and subjective well-being: The sample case of caregiving for a family member with mental illness. Journal of Personality and Social Psychology, 100(5), 934–946. https://doi.org/10.1037/a0022873
Wrosch, C., Barlow, M. A., & Kunzmann, U. (2018). Age-related changes in older adults’ anger and sadness: The role of perceived control. Psychology and Aging, 33(2), 350.
Wrosch, C., & Miller, G. E. (2009). Depressive symptoms can be useful: Self-regulatory and emotional benefits of dysphoric mood in adolescence. Journal of Personality and Social Psychology, 96(6), 1181–1190. https://doi.org/10.1037/a0015172
Wrosch, C., Rueggeberg, R., & Hoppmann, C. A. (2013). Satisfaction with social support in older adulthood: The influence of social support changes and goal adjustment capacities. Psychology and Aging, 28(3), 875–885. https://doi.org/10.1037/a0032730
Wrosch, C., & Sabiston, C. M. (2013). Goal adjustment, physical and sedentary activity, and well-being and health among breast cancer survivors: Goal adjustment, lifestyle activity, and well-being and health. Psycho-Oncology, 22(3), 581–589. https://doi.org/10.1002/pon.3037
Wrosch, C., & Scheier, M. F. (2020). Adaptive self-regulation, subjective well-being, and physical health: The importance of goal adjustment capacities (pp. 199–238). Elsevier.
Wrosch, C., Scheier, M. F., Carver, C. S., & Schulz, R. (2003a). The importance of goal disengagement in adaptive self-regulation: When giving up is beneficial. Self and Identity, 2(1), 1–20. https://doi.org/10.1080/15298860309021
Wrosch, C., Scheier, M. F., Miller, G. E., Schulz, R., & Carver, C. S. (2003b). Adaptive self-regulation of unattainable goals: Goal disengagement, goal reengagement, and subjective well-being. Personality and Social Psychology Bulletin, 29(12), 1494–1508. https://doi.org/10.1177/0146167203256921
Yarrington, J. S., Lasser, J., Garcia, D., Vargas, J. H., Couto, D. D., Marafon, T., Craske, M. G., & Niles, A. N. (2021). Impact of the COVID-19 pandemic on mental health among 157,213 Americans. Journal of Affective Disorders, 286, 64–70. https://doi.org/10.1016/j.jad.2021.02.056
Zhu, L., Ranchor, A. V., van der Lee, M., Garssen, B., Sanderman, R., & Schroevers, M. J. (2015). The role of goal adjustment in symptoms of depression, anxiety and fatigue in cancer patients receiving psychosocial care: A longitudinal study. Psychology & Health, 30(3), 268–283. https://doi.org/10.1080/08870446.2014.969263
Funding
This study was supported in part by grant funding from North Dakota State University to Jeremy M. Hamm and Katherine A. Duggan; a National Heart, Lung, and Blood Institute award to (L30HL143741) to Katherine A. Duggan; and by a postdoctoral fellowship to Meaghan A. Barlow from the Social Sciences and Humanities Research Council of Canada.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hamm, J.M., Tan, J.X.Y., Barlow, M.A. et al. Goal adjustment capacities in uncontrollable life circumstances: Benefits for psychological well-being during COVID-19. Motiv Emot 46, 319–335 (2022). https://doi.org/10.1007/s11031-022-09941-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11031-022-09941-6