
Abstract
In December 2019, a new coronavirus, SARS-COV-2, caused a cluster of cases of pneumonia in China, and rapidly spread across the globe. It was declared a pandemic by the World Health Organization on March 11th, 2020. Virtual autopsy by post-mortem CT (PMCT) and its ancillary techniques are currently applied in post-mortem examinations as minimally or non-invasive techniques with promising results. In this narrative review, we speculate on the potentials of PMCT and its ancillary techniques, as a viable investigation technique for analysis of suspected or confirmed SARS-COV-2 deaths. An online literature search was performed by using three prefix search terms (postmortem, post-mortem, post mortem) individually combined with the suffix radiology, imaging, computed tomography, CT and with the search terms ‘SARS-CoV-2’ and ‘COVID-19’ to identify papers about PMCT and its ancillary techniques in SARS-COV-2 positive cadavers. PMCT findings suggestive for pulmonary COVID-19 in deceased positive SARS-COV-2 infection are reported in the literature. PMCT ancillary techniques were never applied in such cases. PMCT imaging of the lungs has been proposed as a pre-autopsy screening method for SARS-COV-2 infection. Further studies are needed to ascertain the value of PMCT in determining COVID-19 as the cause of death without autopsy histopathological confirmation. We advocate the application of PMCT techniques in the study of ascertained or suspected SARS-COV-2 infected deceased individuals as a screening technique and as a method of post-mortem investigation, to augment the numbers of case examined and significantly reducing infection risk for the operators.
Similar content being viewed by others


Introduction
In December 2019, a new coronavirus was the cause of a cluster of cases of pneumonia that originated in China, and subsequently spread across the world. It was declared a pandemic by the World Health Organization (WHO) on March 11th, 2020 [1]. The coronavirus family comprises several viruses that cause serious human diseases including Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS) [2]. The SARS-coronavirus-2 (SARS-COV-2) causes an illness in humans named as coronavirus disease 2019 (COVID-19) by WHO [1, 3].
Although the upper respiratory tract and lungs represent the predominant site of entry and replication of SARS-COV-2, other replication sites such as endothelial cells and the kidney have been suggested [4, 5].
The major manifestations of COVID-19 involve the respiratory tract; however, extrapulmonary manifestations of COVID-19 infection, particularly neurological manifestations, have been well described in the literature [6, 7].
Until now, several studies based on autopsy cases have been published about the histopathological findings in SARS-COV-2 infection [8,9,10,11]. Autopsy or other alternative post-mortem investigations are essential to elucidate pathophysiological mechanisms of SARS-COV-2 and contributed enormously to advances in the prevention and treatment of patients with COVID-19.
In these scenarios, while performing complete autopsy is of outmost importance, the contamination risk of infection for operators during body sectioning is a critical issue. Despite recommendations from some authors and scientific societies, such as the Italian Society of Anatomical Pathology (SIAPEC), to restrict autopsies to selected cases at a first time, many forensic institutions have continued to regularly perform autopsies since the beginning of the pandemic [12, 13]. However, if death occurred in a person with suspected or confirmed SARS-COV-2 infection, but is involved in forensic investigation, performing an autopsy is necessary in most cases. The roles, indications and guidelines for the correct management of potential infectious pathogens applied in clinical and research practice in microbiology laboratories have been translated to mortuary setting to reduce transmission risk of these pathogens during and after post-mortem examinations.
In the deceased where SARS–COV-2 is suspected or ascertained, as well as for other high risk of infection pathogens, some guidelines for safe autopsy procedures have been defined in Italy by the Italian National Institute of Health (INIH) [14].
Essentially, the precautions indicated by INIH and other international health organizations [15, 16] are related to the environment where the autopsy is performed, protection of the operator, selection of the operator and knowledge of the case history.
Thus, because autopsies performed on people with high risk of infection request specific procedures and environmental conditions in the autopsy room, high numbers of autopsies on SARS-COV-2 cases were difficult to achieve, at least during the first peak of the pandemic.
The term “Virtual autopsy” or “Virtopsy®” was defined in 2002 by Prof. Thali et al. at the Institute of Forensic Medicine of the University of Bern, Switzerland, as the set of imaging techniques used on a cadaver for forensic purposes [17, 18]. The fundamental basis for a modern virtual autopsy is undoubtedly a whole-body post-mortem CT (PMCT) scan in high-resolution due to the ability to neglect radiation exposure and the absence of motion artifacts [19, 20]. Although PMCT is considered very useful to analyze violent deaths due to the optimal visualization of skeletal lesions, intravascular gas, foreign bodies, this technique shows limitations in investigating "natural" deaths, due to its poor ability in differentiating soft tissue interfaces and in documenting vascular alterations [17]. In 2005, PMCT angiography, firstly introduced by Jackowski et al. [21] and after improved by variating the technique and the type of intravascular contrast media [22,23,24], overcame most limitations in documenting vascular alterations.
However, a significant limit of PMCT remained the absence of body samples for histopathological, microbiological or toxicological analysis. To overcome this limit, by 2007, post-mortem percutaneous biopsy [25,26,27] proved to successively provide specimens suitable for histological examination.
Since then, post-mortem imaging techniques, primarily PMCT, have also been successfully applied to the investigation of non-forensic cases. In fact, these post-mortem modalities have been used for pathological investigations and even in veterinary settings [28,29,30].
In this narrative review, we speculate on the potentials of the modern techniques of virtual autopsy by PMCT and its ancillary techniques, mainly PMCT angiography and percutaneous biopsy, as a viable non-invasive, or minimally invasive technique for analysis of suspected or confirmed SARS-COV-2 deaths, to favor the reduction of operator risk of infection and to increase the availability of post-mortem data, on a histopathological level in individuals who died with SARS-COV-2 infection. PMCT findings in deceased positive SARS-COV-2 infection, especially focusing on the lungs, as reported in the current available literature are also presented. Finally, possible applications of ancillary to PMCT techniques in post-mortem investigations on SARS-COV-2 cases are also discussed. With the aim to cover the entire pertinent literature, one of the authors, a board-certified radiologist and forensic pathologist with more than fifteen years of experience in post-mortem imaging, independently searched in two databases, PubMed and Google Scholar. Three prefix search terms (postmortem, post-mortem, post mortem) were individually combined with the suffix radiology, imaging, computed tomography, CT and with the search terms ‘SARS-CoV-2’ and ‘COVID-19’. The inclusion criteria were all types of articles and related only to humans. The exclusion criteria were articles for which full text was not available, were not in English. From the articles retrieved in the first round of search, additional references were examined by a manual search among the cited references.
CT findings in living patients
It is well demonstrated that SARS-COV-2 affects principally the lungs. Based on the available biopsy or autopsy studies, pulmonary pathology [11, 31] in SARS-COV 2 infection is represented by diffuse alveolar damage due to the development of hyaline membranes, macrophage activation in the air spaces, and thickening of the alveolar wall.
Many clinical studies have reported different CT patterns of pulmonary involvement [32,33,34,35,36,37,38,39]. According to the recent literature [38, 39], the most typical of chest CT findings in COVID-19 patients are bilateral lung involvement by ground-glass opacity (GGO) or mixed GGO and consolidation, thickened interlobular septa, crazy-paving pattern, vascular enlargement, air bronchogram sign, peripheral distribution, and left and right lower lobes involvement. However, the same pattern identified as typical for COVID-19 in the lungs, is common with the lung CT pattern caused by other viral pathogens, for example virus such as H7N9, H1N1 virus infection, SARS, MERS, and avian influenza A (H5N1) [40,41,42,43], or other sources of lung pathology such as drug reactions. Nevertheless, chest CT scan is considered an important part of disease diagnosis for patients suspected of having COVID-19, especially those with negative initial reverse-transcription polymerase chain reaction (RT-PCR) screening [44]. In fact, given the limited number of RT-PCR kits in many centers and the likelihood of false negative RT-PCR results, the National Health Commission of the People's Republic of China, has suggested CT as a major modality for diagnosis, even before receiving the RT-PCR tests [45].
Other organs are affected by SARS-COV-2 due to direct attack by the virus or through an indirect mechanism mediated by inflammation and coagulation mediators [46, 47]. The lymph nodes, heart, kidneys, spleen, liver, gastrointestinal tract and brain have all been indicated as organs affected by multiorgan dysfunction in COVID-19 disease. Some studies report CT findings in extrapulmonary manifestations of COVID-19 [46], mainly focusing on the brain and the bowel. In the brain, due to potential endothelial damage, SARS-COV-2 may cause hemorrhagic lesions [48, 49]. Possible CT manifestations of SARS-COV-2 involvement of the brain are hypodensity within the bilateral medial thalami on the head CT and hemorrhagic lesions [50, 51]. Regarding the gastrointestinal tract, non-specific findings such as distended fluid filled small and large bowel loops and surrounding stranding, intestinal wall thickening on clinical non-enhanced CT have been reported, as the expression of parietal bowel damage in COVID-19 [46, 52,53,54,55]. Uncommonly, mediastinal lymphadenopathy with lymph node enlargement potentially detected by CT imaging has been reported in the literature in critically ill COVID-19 patients, as an expression of the inflammatory response to the infection [56]. SARS-COV-2 was also detected in the liver cells and microvesicular steatosis of moderate entity and mild lobular and portal inflammatory activity were reported in some histopathological studies on SARS-COV-2 patients [46]. The literature suggests that 71,4% of non-survivors of COVID-19 suffered from disseminated intravascular coagulation, with abnormal coagulation results in later stages of the disease [57]. In critically ill COVID-19 patients two types of pathologic coagulation processes can be identified, one involving the microcirculation of the lungs and other organs causing microvascular clots [58], and the other affecting the systemic circulation with the potential development of large vessel thrombosis and major thromboembolic events, including pulmonary embolism [59,60,61].
Potential use of postmortem CT in SARS-COV-2 positive deaths
The literature research of this narrative review retrieved papers regarding the use of PMCT in SARS-COV-2 positive cadavers [62,63,64,65,66,67,68,69,70]. It is interesting to note that all the selected papers were focused on PMCT appearances of SARS-COV-2 lung disease. Papers about extrapulmonary manifestations of COVID-19 on PMCT or about ancillary PMCT techniques (i.e., PMCT angiography and PMCT guided percutaneous biopsy) applied in SARS-COV-2 positive cadavers were not published.
PMCT of the lungs
The potentials of PMCT in identifying significant pulmonary alterations in post-mortem investigations are well known [71,72,73]. The presence of air in the lungs provides an intrinsic contrast, that renders the lungs one of the organs best imaged on non-enhanced CT in clinical and post-mortem setting. PMCT imaging of the lungs is considered a valuable tool in forensic investigations, and it is employed as a post-mortem method of analysis as an adjunctive or even substitutive tool for autopsy [74]. As well as in other organs, in the pulmonary parenchyma the formation of internal livors affects their PMCT imaging, even more than in other organs. Internal hypostases in the lungs appear as an attenuation gradient with areas of grater opacity mainly of ground glass type, localized in dependent regions of the lungs (e.g., positions that may vary depending on the decubitus after death) [71].
These normal post-mortem alterations on PMCT imaging might mask an underlying COVID-19 lung involvement. This is theoretically more probable in initial stages of lung pathology, when few and scanty areas of ground glass opacity could be in dorsal, peripheral regions, eventually in the inferior lobes, thus with the same distribution of internal livors. If we do not take in to account the increase of the risk of infection, forced mechanical ventilation of cadaveric lungs might be proposed to improve the detection of COVID-19 related lung alterations. In fact, this technique has been proved to be a valuable method to reduce PMCT findings related to hypostases in the lungs and to enhance relevant pathological pulmonary PMCT findings [75].
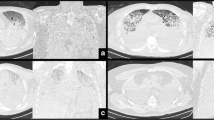
The presented review of the literature confirmed the value of PMCT in cadavers positive for SARS-COV-2 infection. The most common findings on PMCT reported in the literature as the expression of severe pulmonary COVID-19, as it occurs in clinical setting, were bilateral, mixed pattern of GGOs, commonly with crazy paving pattern, and consolidations, in either a diffuse or a peripheral distribution [62,63,64,65,66,67,68,69,70] (Fig. 1 exemplar). An adjunctive, even more not specific pattern was diffuse consolidation and GGO of both lungs [67, 69, 70], described by O’Donnell as “dense airless lungs”, attributed to advanced COVID-19 pneumonitis in clinical setting [32,33,34,35,36,37,38,39], can be interpreted as a common final common pathway in respiratory illness related to severe lung involvement by the pathogen, resembling adult respiratory distress syndrome (ARDS).

Case example of advanced COVID-19 pulmonary involvement on PMCT imaging. Axial PMCT images at the level of the thorax in a deceased with ascertained SARS-COV-2 infection. PMCT images (a, b) show bilateral massive involvement of pulmonary parenchyma with diffuse crazy paving pattern and multiple areas of consolidations, with some air bronchogram (b)
In the previous publications about PMCT alterations of the lungs in SARS-COV-2 positive cases, this post-mortem investigation tool was basically proposed as a screening method for SARS-COV-2 infection in cadavers [62,63,64,65,66,67,68, 70]. Regarding the possibility to attribute the cause of death based on PMCT imaging, it was most commonly [68,69,70] retained that there is currently insufficient published literature and the findings reported for assessment of SARS-CoV-2 infection of the lungs using PMCT are not sufficiently specific to propose this post-mortem imaging technology as an alternative to autopsy and histopathological, and microbiological analysis.
PMCT of other organs
As previously mentioned, other organs are affected by SARS-COV-2 due to direct attack or by indirect mechanisms [6, 46, 47].
Although no PMCT imaging findings corresponding to these pathological alterations have yet been reported, most of the ante-mortem extrapulmonary CT alterations suggested in the literature as related to SARS-COV-2 infection, might be theoretically identified in PMCT imaging. Namely, in the brain as well as in clinical CT, the endothelial damage caused by SARS-COV-2 infection might be expressed by ischemic or hemorrhagic lesions [48,49,50,51].
Other possible extrapulmonary CT findings may be mediastinal lymphadenopathy with lymph node enlargement [56], large bowel loops and surrounding stranding, intestinal wall thickening [46, 52,53,54,55], diffuse hypodensity of the liver due to non-specific steatosis [46]. Regarding the CT imaging findings related to disseminated intravascular coagulation elicited by SARS-COV-2 in critically ill patients [57,58,59,60,61], it is of interest to note that unenhanced PMCT has been used to document central pulmonary embolism based on the shape of the vascular content within the pulmonary trunk and arteries [76, 77]. Moreover, it has been verified that distension of the inferior vena cava on PMCT suggests the presence of pulmonary thromboembolism with a specificity of 83% and a sensitivity of 54% [76].
PMCT angiography
PMCT angiography has been introduced in virtual autopsy as a complementary technique; this technique adds crucial information about vascular bed in non-decomposed cadavers, enhancing virtual autopsy, particularly in natural deaths [21,22,23,24, 78]. Some studies have demonstrated the capability of PMCT angiography to document central and paracentral pulmonary thromboembolism [22, 79], and a complete concordance with autopsy results and histological analysis was verified. Also, deep venous thrombosis has been demonstrated in some cases of PMCT angiography with known pulmonary embolism [79]. Otherwise, the development of small post-mortem clots and/or the presence of possible minute filling defects due to artifacts generally impairs the correct identification of more peripheral pulmonary embolism [22].
Thus, in cases of suspected lethal pulmonary embolism, the diagnostic accuracy of PMCT angiography in diagnosing pulmonary embolism is not completely proven, due to the absence of large cadaveric studies. Furthermore, post-mortem clots and artifacts may compromise the accuracy of this post-mortem imaging technique in demonstrating pulmonary embolism. In any case, PMCT angiography can be suggested as a viable technique for detecting central and paracentral pulmonary embolism or other major thrombotic or thromboembolic phenomena in a minimally invasive manner in deceased individuals with COVID-19. Nevertheless, the reduced ability of PMCT angiography to demonstrate microvascular thrombosis and embolism renders the histological analysis more desirable.
PMCT-guided biopsy
In the setting of minimally invasive autopsy, post-mortem multiorgan percutaneous biopsies have already been successfully applied to post-mortem investigations of three cases of deceased COVID-19 patients [80]. Post-mortem percutaneous biopsies with PMCT guidance may represent a useful technique for focused minimally invasive post-mortem investigations in deceased individuals with ascertained or suspected SARS-COV-2 infection. In this scenario, post-mortem percutaneous biopsies may permit to overcome the above-mentioned limitations of virtual autopsy with unenhanced PMCT or also with PMCT angiography, by providing tissue and body fluid samples for histological, immunohistochemical, microbiological and toxicological analysis.
Advantages of PMCT in SARS-COV-2 infected deaths
SARS-COV 2 infection is the cause of severe disease with a rapid pandemic diffusion
In the post-mortem setting, Italian National Institute of Health (INIH) has underlined the importance of histopathological, microbiological and virologic analysis on tissue and biological specimens of deceased individuals with ascertained and suspected SARS-COV-2 infection. The aim for autopsy procedure on ascertained cases of COVID-19 is mainly to help in understanding pathophysiological mechanisms of SARS-COV-2 which in turn may contribute enormously to advances in prevention and treatment of patients with COVID-19. On the other hand, the contamination risk for operators during body sectioning is equally a crucial issue, and INIH and other health institutions worldwide have advocated the limitation of body dissections in ascertained and, particularly, in suspected SARS-COV-2 deceased patients. Moreover, due to high mortality rates in many regions of Italy and worldwide, especially in the first peak of pandemic, the large number of deceased individuals to be examined in addition to the proposition to reduce infective risk for health operators undoubtedly limits the rates of autopsy on SARS-COV-2 infected individuals. Furthermore, during the first peak of pandemic, every cadaver to be dissected, also for forensic purposes, must be considered as potentially infected and must undergo post-mortem management of potentially high grade HG3 pathogens.
Other limits to full autopsy are the availability of adequate mortuary rooms, protective devices, and trained operators to guarantee acceptable reduction of risk of transmission of infection to third parties. The same INIH in the document reporting indications about autopsy procedures [14] states “in patients dying with SARS-CoV-2 infection, the autopsies can confirm laboratory and radiological findings […]”.
Although in a recent systematic review about the development of forensic imaging in Italy an increase of the use of these techniques, particularly PMCT, has been observed in the last years, the literature demonstrated that imaging techniques are not yet exhaustively adopted by the Italian forensic community, and that most publications are from authors affiliated with university groups of research [81]. However, due to the wide diffusion of CT in the Italian territory both in university and in extra-university context, we are convinced that PMCT can represent the technique of choice for post-mortem investigations in pandemic emergencies.
With this contribution, we suggest the use of these post-mortem investigation techniques in cadavers of ascertained and suspected SARS-COV-2 infected individuals.
The advantages are several including that these procedures, minimally or non-invasive, can significantly reduce the risk of infection of the operators. Above all, if exclusively a whole body PMCT is performed, preliminary information about a potential COVID-19 lung disease is achievable, particularly in cadavers where clinical information before death is not available and the complete results of viral nose and throat swab are still not available. Moreover, a whole body PMCT is rapid and does not require specific environmental conditions, different to those normally applicable on living patients. Thus, the numbers of cadavers undergoing post-mortem analysis could be significantly increased.
Moreover, in ascertained cases of death due to COVID-19 focused, eventually CT guided, post-mortem percutaneous biopsies may improve the understanding of this lethal pathology with important impact on prevention and treatment, but with consistent reduction of infection for the operators unlike in classical autopsy techniques.
Finally, a general advantage of this post-mortem technique is to provide an objective data set available for further analysis.
Conclusions
For all the aforementioned reasons, we advocate the application of PMCT virtual autopsy techniques in the study of ascertained or suspected SARS-COV-2 infected deceased individuals as a screening technique and as a method of post-mortem investigation. These techniques might be able to provide significant information about COVID-19 on many deceased patients while significantly reducing infection risk for the operators.
References
World Health Organization (2020) Rolling updates on coronavirus disease (COVID-19). https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen. Accessed January 2021
Holmes KV (2003) SARS-associated coronavirus. N. Engl. J. Med. 348(20):1948–1951
World Health Organization, WHO Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020 (2020) https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020. Accessed January 2021
Su H, Yang M, Wan C et al (2020) Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. https://doi.org/10.1016/j.kint.2020.04.003
Kissling S, Rotman S, Gerber C et al (2020) Collapsing glomerulopathy in a COVID-19 patient. Kidney Int. 98(1):228–231
Yazdanpanah F, Garg A, Shadman S, Asmarz HY (2021) Literature review of COVID-19, pulmonary and extrapulmonary disease. Am. J. Med. Sci. 361(5):567–574
Finsterer J, Scorza FA (2021) Clinical and pathophysiologic spectrum of neuro-COVID. Mol. Neurobiol. 8:1–5
Vasquez-Bonilla WO, Orozco R, Argueta V, Sierra M, Zambrano LI, Muñoz-Lara F, López-Molina DS, Arteaga-Livias K, Grimes Z, Bryce C, Paniz-Mondolfi A, Rodríguez-Morales AJ (2020) A review of the main histopathological findings in coronavirus disease 2019. Hum. Pathol. 105:74–83
Wichmann D (2020) Autopsy findings and venous thromboembolism in patients with COVID-19. Ann. Intern. Med. 173(12):1030
Kirschenbaum D, Imbach LL, Rushing EJ, Frauenknecht KBM, Gascho D, Ineichen BV, Keller E, Kohler S, Lichtblau M, Reimann RR, Schreib K, Ulrich S, Steiger P, Aguzzi A, Frontzek K (2021) Intracerebral endotheliitis and microbleeds are neuropathological features of COVID-19. Neuropathol. Appl. Neurobiol. 47(3):454–459
Maiese A, Manetti AC, La Russa R, Di Paolo M, Turillazzi E, Frati P, Fineschi V (2021) Autopsy findings in COVID-19-related deaths: a literature review. Forensic. Sci. Med. Pathol. 17(2):279–296
Sapino A, Facchetti F, Bonoldi E, Gianatti A, Barbareschi M, Italiana S, di AnatomiaPatologica e Citologia - SIAPEC (2020) The autopsy debate during the COVID-19 emergency: the Italian experience. Virchows Arch. 476(6):821–823
Sperhake JP (2020) Autopsies of COVID-19 deceased? Absolutely! Leg. Med. (Tokyo) 47:101769
Rapporto ISS COVID-19 n. 6/2020 - Procedura per l’esecuzione di riscontri diagnostici in pazienti deceduti con infezione da SARSCoV-2. Versione del 27 marzo 2020. https://www.iss.it/documents/20126/0/Rapporto+COVID19+n.+6_2020+Autopsie+v27+marzo.pdf/c4b363a1-a246-c36c-d007-ae24ed7e648b?t=1585307031219. Accessed January 2021
Osborn M, Lucas S, Stewart R, et al (2020) Autopsy practice relating to possible cases of COVID-19 (2019-nCov, novel coronavirus from China 2019/2020) secondary autopsy practice relating to possible cases of COVID-19 (2019-nCov, novel coronavirus from China 2019/2020). https://www.rcpath.org/uploads/assets/d5e28baf-5789-4b0f-acecfe370eee6223/fe8fa85a-f004-4a0c-81ee4b2b9cd12cbf/Briefing-on-COVID-19-autopsy-Feb-2020.Pdf. Accessed January 2021
Centers for disease control and prevention (2020). Collection and Submission of Postmortem Specimens from Deceased Persons with Known or Suspected COVID-19, March 2020 (Interim Guidance). https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html. Accessed January 2021
Thali MJ, Yen K, Schweitzer W et al (2003) Virtopsy, a new imaging horizon in forensic pathology: virtual autopsy by postmortem multislice computed tomography (MSCT) and magnetic resonance imaging (MRI)–a feasibility study. J. Forensic. Sci. 48(2):386–403
Dirnhofer R, Jackowski C, Vock P, Potter K, Thali MJ (2006) VIRTOPSY: minimally invasive, imaging-guided virtual autopsy. Radiographics 26(5):1305–1333
Filograna L, Pugliese L, Muto M et al (2019) A practical guide to virtual autopsy: why, when and how. Semin. Ultrasound. CT MR 40(1):56–66
Gascho D, Thali MJ, Niemann T (2018) Post-mortem computed tomography: technical principles and recommended parameter settings for high-resolution imaging. Med. Sci. Law 58(1):70–82
Jackowski C, Sonnenschein M, Thali MJ et al (2005) Virtopsy: postmortem minimally invasive angiography using cross section techniques–implementation and preliminary results. J. Forensic. Sci. 50(5):1175–1186
Ross S, Spendlove D, Bolliger S et al (2008) Postmortem whole-body CT angiography: evaluation of two contrast media solutions. AJR Am. J. Roentgenol. 190(5):1380–1389
Grabherr S, Doenz F, Steger B et al (2011) Multi-phase post-mortem CT angiography: development of a standardized protocol. Int. J. Legal. Med. 125(6):791–802
Péporté ARJ, Gascho D, Stamou S, Bensler S, Thali MJ, Leschka S, Flach PM (2020) Evaluation of an acetated Ringer-based contrast material mixture for postmortem computed tomography angiography. Diagn. Interv. Imaging 101(7–8):489–497
Aghayev E, Thali MJ, Sonnenschein M, Jackowski C, Dirnhofer R, Vock P (2007) Post-mortem tissue sampling using computed tomography guidance. Forensic. Sci. Int. 166:199–203
Bolliger SA, Filograna L, Spendlove D, Thali MJ, Dirnhofer S, Ross S (2010) Post-mortem image-guided biopsy as an adjuvant to minimal invasive autopsy with computed tomography and post-mortem angiography: a feasibility study. AJR 195:1051–1056
Filograna L, Bolliger SA, Kneubuehl B, Jackowski C, Hatch GM, Thali MJ (2012) A minimally invasive technique for the detection and analysis of pulmonary fat embolism: a feasibility study. J. Forensic. Sci. 57(5):1329–1335
Blokker BM, Wagensveld IM, Weustink AC, Oosterhuis JW, Hunink MG (2016) Non-invasive or minimally invasive autopsy compared to conventional autopsy of suspected natural deaths in adults: a systematic review. Eur. Radiol. 26(4):1159–1179
Bolliger SA, Thali MJ (2009) Forensic Veterinary Radiology. In: Thali MJ, Dirnhofer R, Vock P (eds) The Virtopsy Approach: 3D Optical and Radiological Scanning and Reconstruction in Forensic Medicine. CRC Press, Boca Raton, pp 491–499
Ibrahim AO, Zuki ABM, Noordin MM (2012) Applicability of virtopsy in veterinary practice: a short review. Pertanika J. Trop. Agric. Sci. 35(1):1–8
Xu Z, Shi L, Wang Y et al (2020) Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 8(4):420–422
Chung M, Bernheim A, Mei X et al (2020) CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 295(1):202–207
Kong W, Agarwal PP (2020) Chest imaging appearance of COVID-19 infection. Radiol. Cardiothorac. Imaging 2(1):e200028
Bernheim A, Mei X, Huang M et al (2020) Chest CT findings in coronavirus disease-19 (COVID-19): relationship to duration of infection. Radiology 295(3):200463
Pan F, Ye T, Sun P et al (2020) Time course of lung changes at chest CT during recovery from coronavirus disease 2019 (COVID-19). Radiology 295(3):715–721
Bai HX, Hsieh B, Xiong Z et al (2020) Performance of radiologists in differentiating COVID-19 from non-COVID-19 viral pneumonia at chest CT. Radiology 296(2):E46–E54
Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A (2020) Coronavirus disease 2019 (COVID-19): a systematic review of imaging findings in 919 patients. AJR Am. J. Roentgenol. 215(1):87–93
Karimian M, Azami M (2021) Chest computed tomography scan findings of coronavirus disease 2019 (COVID-19) patients: a comprehensive systematic review and meta-analysis. Pol. J. Radiol. 86:e31–e49
Zhou X, Pu Y, Zhang D, Xia Y, Guan Y, Liu S, Fan L (2021) CT findings and dynamic imaging changes of COVID-19 in 2908 patients: a systematic review and meta-analysis. Acta Radiol. https://doi.org/10.1177/0284185121992655
Wong K-t, Antonio GE, Hui DS et al (2004) Severe acute respiratory syndrome: thin-section computed tomography features, temporal changes, and clinicoradiologic correlation during the convalescent period. J. Comput. Assist. Tomogr. 28:790–795
Qureshi NR, Hien TT, Farrar J et al (2006) The radiologic manifestations of H5N1 avian influenza. Journal of thoracic imaging. J. Thorac. Imaging 21:259–264
Paul NS, Roberts H, Butany J et al (2004) Radiologic pattern of disease in patients with severe acute respiratory syndrome: the Toronto experience. Radiographics 24:553–563
Das KM, Lee EY, Langer RD et al (2016) Middle east respiratory syndrome coronavirus: what does a radiologist need to know? AJR Am. J. Roentgenol. 206:1193–1201
Xie X, Zhong Z, Zhao W et al (2020) Chest CT for typical 2019-nCoV pneumonia: relationship to negative RT-PCR testing. Radiology 296:E41–E45
National Health Commission of the People’s Republic of China. (2020) China’s Hubei reports jump in new cases of COVID-19 after diagnosis criteria revision. http://en.nhc.gov.cn/2020-02/13/c_76515.htm. Accessed January 2021
Behzad S, Aghaghazvini L, Radmard AR, Gholamrezanezhad A (2020) Extrapulmonary manifestations of COVID-19: Radiologic and clinical overview. Clin. Imaging 66:35–41
Mehta OP, Bhandari P, Raut A, Kacimi SEO, Huy NT (2021) Coronavirus disease (COVID-19): comprehensive review of clinical presentation. Front. Public Health 8:582932
Huang C, Wang Y, Li X et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223):497–506
Baig AM, Khaleeq A, Ali U, Syeda H (2020) Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chem. Neurosci. 11(7):995–998
Sharifi-Razavi A, Karimi N, Rouhani N (2020) COVID-19 and intracerebral haemorrhage: causative or coincidental? New Microbes New Infect. 35:100669
Poyiadji N, Shahin G, Noujaim D, Stone M, Patel S, Griffith B (2020) COVID-19-associated acute hemorrhagic necrotizing encephalopathy: imaging features. Radiology 296(2):E119–E120
Horvat N, Pinto PVA, Araujo-Filho JAB, Santos JMMM, Dias AB, Miranda JA, de Oliveira CV, Barbosa CS, Morais TC, Assuncao AN Jr, Nomura CH, Viana PCC (2021) Abdominal gastrointestinal imaging findings on computed tomography in patients with COVID-19 and correlation with clinical outcomes. Eur. J. Radiol. Open 8:100326
Abobaker A, Raba AA, Alzwi A (2020) Extrapulmonary and atypical clinical presentations of COVID-19. J. Med. Virol. 92:2458–2464
Pan L, Mu M, Yang P, Sun Y, Wang R, Yan J, Li P, Hu B, Wang J, Hu C, Jin Y, Niu X, Ping R, Du Y, Li T, Xu G, Hu Q, Tu L (2020) Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: a descriptive, cross-sectional. Multicenter Study Am. J. Gastroenterol. 115(5):766–773
Chan KH, Lim SL, Damati A, Maruboyina SP, Bondili L, Abu Hanoud A, Slim J (2020) Coronavirus disease 2019 (COVID-19) and ischemic colitis: an under-recognized complication. Am. J. Emerg. Med. 38:2758.e1-2758.e4
Valette X, du Cheyron D, Goursaud S (2020) Mediastinal lymphadenopathy in patients with severe COVID-19. Lancet Infect. Dis. 20(11):1230
Zhou F, Yu T, Du R et al (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395(10229):1054–1062
Varga Z, Flammer AJ, Steiger P et al (2020) Endothelial cell infection and endotheliitis in COVID-19. Lancet 395:1417–1418
Klok FA, Kruip MJHA, van der Meer NJM et al (2020) Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 191:145–147
Poissy J, Goutay J, Caplan M, Parmentier E, Duburcq T, Lassalle F, Jeanpierre E, Rauch A, Labreuche J, Susen S (2020) Lille ICU haemostasis COVID-19 group pulmonary embolism in patients with COVID-19: awareness of an increased prevalence. Circulation 142(2):184–186
Léonard-Lorant I, Delabranche X, Séverac F, Helms J, Pauzet C, Collange O, Schneider F, Labani A, Bilbault P, Molière S, Leyendecker P, Roy C, Ohana M (2020) Acute pulmonary embolism in patients with COVID-19 at CT angiography and relationship to d-Dimer levels. Radiology 296(3):E189–E191
Schweitzer W, Ruder T, Baumeister R et al (2020) Implications for forensic death investigations from first Swiss post-mortem CT in a case of non-hospital treatment with COVID-19. Forensic Imaging. https://doi.org/10.1016/j.fri.2020.200378
Kniep I, Heinemann A, Edler C, Sperhake JP, Püschel K, Ondruschka B, Schroeder AS (2021) COVID-19 lungs in post-mortem computed tomography. Rechts (Berl). https://doi.org/10.1007/s00194-021-00462-z
Ducloyer M, Gaborit B, Toquet C et al (2020) Complete post-mortem data in a fatal case of COVID-19: clinical, radiological and pathological correlations. Int. J. Legal Med. 134(6):2209–2214
Helmrich E, Decker L, Adolphi N, Makino Y (2020) Postmortem CT lung findings in decedents with Covid-19: a review of 14 decedents and potential triage implications. Forensic Imaging. https://doi.org/10.1016/j.fri.2020.200419
Fitzek A, Sperhake J, Edler C, Schröder AS, Heinemann A, Heinrich F, Ron A, Mushumba H, Lütgehetmann M, Püschel K (2020) Evidence for systematic autopsies in COVID-19 positive deceased: case report of the first German investigated COVID-19 death. Rechtsmedizin (Berl). https://doi.org/10.1007/s00194-020-00401-4
De-Giorgio F, Cittadini F, Cina A, Cavarretta E, Biondi-Zoccai G, Vetrugno G, Natale L, Colosimo C, Pascali VL (2021) Use of post-mortem chest computed tomography in Covid-19 pneumonia. Forensic. Sci. Int. 325:110851
Williams AS, Dmetrichuk JM, Kim P, Pollanen MS (2021) Postmortem radiologic and pathologic findings in COVID-19: the Toronto experience with pre-hospitalization deaths in the community. Forensic. Sci. Int. 322:110755
Filograna L, Manenti G, Arena V, Dell’Aquila M, Pascali VL, Natale L, Colosimo C, Grassi S, Floris R, Oliva A (2021) Claimed medical malpractice in fatal SARS-CoV-2 infections: the importance of combining ante- and post-mortem radiological data and autopsy findings for correct forensic analysis. Forensic Imaging. https://doi.org/10.1016/j.fri.2021.200454
O’Donnell C, Iles L, Woodford N (2021) Post-mortem CT lung findings at a medicolegal institute in SARS-CoV-2 RT-PCR positive cases with autopsy correlation. Forensic. Sci. Med. Pathol. 17(4):611–620
Filograna L, Thali MJ (2017) Post-mortem CT imaging of the lungs: pathological versus non-pathological findings. Radiol. Med. 122(12):902–908
Filograna L, Bolliger SA, Ross SG, Ruder T, Thali MJ (2011) Pros and cons of post-mortem CT imaging on aspiration diagnosis. Leg. Med. (Tokyo) 13(1):16–21
Filograna L, Ross S, Bolliger S, Germerott T, Preiss U, Flach PM, Thali M (2011) Blood aspiration as a vital sign detected by postmortem computed tomography imaging. J. Forensic. Sci. 56(3):630–637
Filograna L, Tartaglione T, Vetrugno G et al (2015) Freshwater drowning in a child: a case study demonstrating the role of post-mortem computed tomography. Med. Sci. Law 55(4):304–311
Germerott T, Preiss US, Ebert LC, Ruder TD, Ross S, Flach PM, Ampanozi G, Filograna L, Thali MJ (2010) A new approach in virtopsy: Postmortem ventilation in multislice computed tomography. Leg. Med. (Tokyo) 12(6):276–279
Mueller SL, Thali Y, Ampanozi G et al (2015) Distended diameter of the inferior vena cava is suggestive of pulmonary thromboembolism on unenhanced post-mortem CT. J. Forensic. Radiol. Imaging 2:10. https://doi.org/10.1016/j.jofri.2014.11.006
Ampanozi G, Held U, Ruder TD et al (2016) Pulmonary thromboembolism on unenhanced postmortem computed tomography: feasibility and findings. Leg. Med. (Tokyo) 20:68–74
Filograna L, Hatch G, Ruder T, Ross SG, Bolliger SA, Thali MJ (2013) The role of post-mortem imaging in a case of sudden death due to ascending aorta aneurysm rupture. Forensic. Sci. Int. 228(1–3):e76-80
Turillazzi E, Frati P, Pascale N et al (2016) Multi-phase post-mortem CT-angiography: a pathologic correlation study on cardiovascular sudden death. J. Geriatr. Cardiol. 13(10):855–865
Yao XH, Li TY, He ZC et al (2020) A pathological report of three COVID-19 cases by minimally invasive autopsies. Zhonghua Bing Li Xue Za Zhi 49(5):411–417
Filograna L, Guglielmi G, Floris R, Marchetti D (2018) The development of forensic imaging in Italy. A systematic review of the literature. J. Forensic. Radiol. Imaging 15:14–20
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
This article does not contain any studies involving human participants performed by any of the authors and informed consent was not requested.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Filograna, L., Manenti, G., Ampanozi, G. et al. Potentials of post-mortem CT investigations during SARS-COV-2 pandemic: a narrative review. Radiol med 127, 383–390 (2022). https://doi.org/10.1007/s11547-022-01457-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-022-01457-w