

Rapid Assessment of COVID-19 Mortality Risk with GASS Classifiers
 ,
,
,
,
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participant Recruitment
2.2. Descriptive Analyses
2.3. Statistical Analysis
2.4. The Clinical-GASS Classifier
2.5. The SVM22-GASS Classifier
2.5.1. Data Preprocessing
2.5.2. Data Augmentation
2.5.3. Feature Selection
2.5.4. Parameter Training
2.5.5. Hyperparameters Optimization
2.5.6. Model Evaluation
2.5.7. Model Interpretation
2.6. Guidelines and Ethical Approval
3. Results
3.1. Descriptive Analyses
3.2. The CCI Classifier
3.3. The Clinical-GASS Classifier
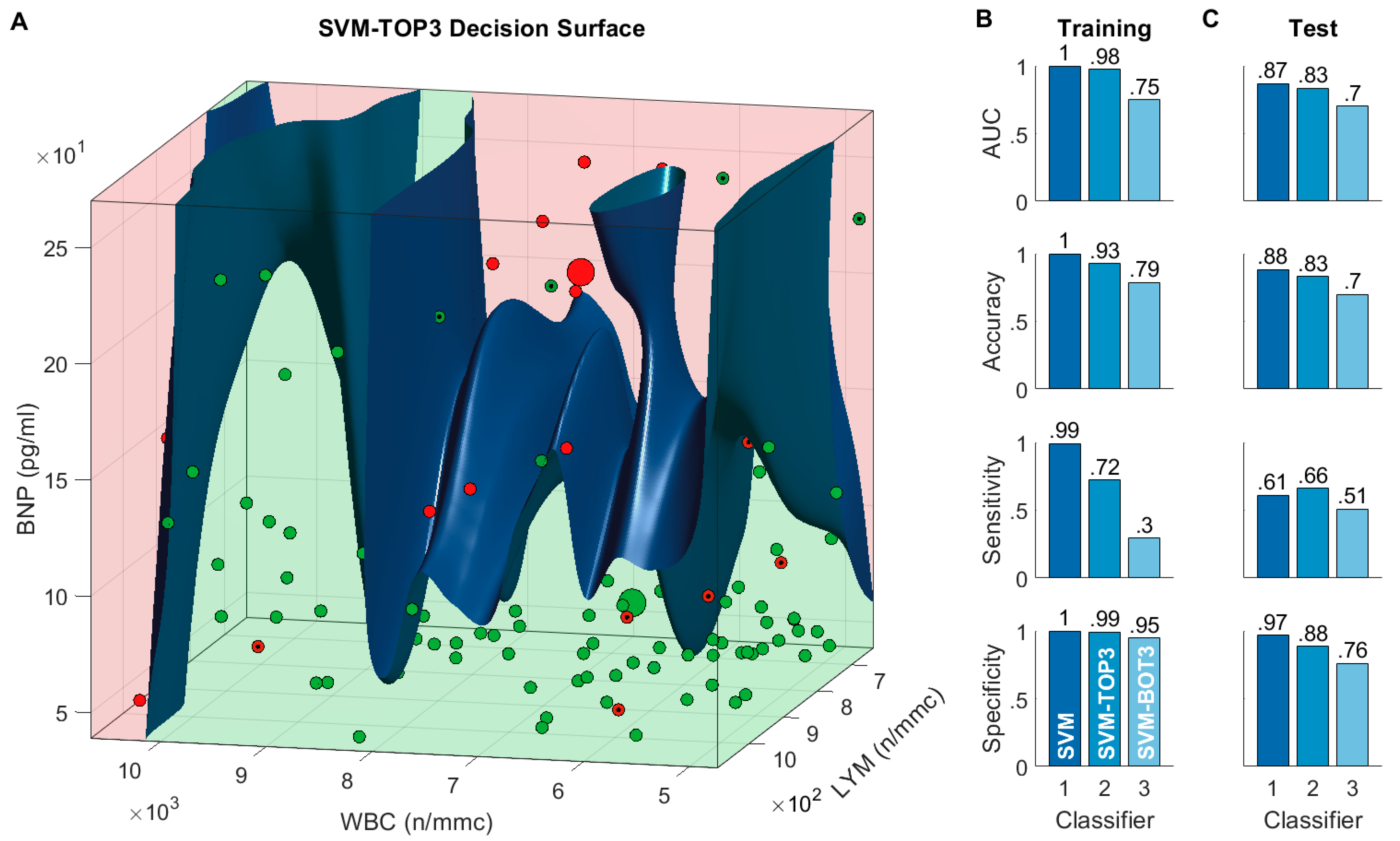
3.4. The SVM22-GASS Classifier
Model Interpretation and Reduced Models
4. Discussion
4.1. Clinical-GASS Score and Risk Factors
4.2. Alternative Clinical Scores
4.3. Interpreting the SVM22-GASS Classifier
4.4. Potential Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Availability of Data and Material
Acknowledgments
Conflicts of Interest
References
- The-nCoV Outbreak Joint Field Epidemiology Investigation Team; Li, Q. An Outbreak of NCIP (2019-NCoV) Infection in China—Wuhan, Hubei Province, 2019–2020. China CDC Wkly. 2020, 2, 79–80. [Google Scholar] [CrossRef]
- COVID—Coronavirus Statistics—Worldometer. Available online: worldometers.info (accessed on 31 January 2023).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, R. Charlson Comorbidity Index. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Tuty Kuswardhani, R.A.; Henrina, J.; Pranata, R.; Anthonius Lim, M.; Lawrensia, S.; Suastika, K. Charlson Comorbidity Index and a Composite of Poor Outcomes in COVID-19 Patients: A Systematic Review and Meta-Analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Christensen, D.M.; Strange, J.E.; Gislason, G.; Torp-Pedersen, C.; Gerds, T.; Fosbøl, E.; Phelps, M. Charlson Comorbidity Index Score and Risk of Severe Outcome and Death in Danish COVID-19 Patients. J. Gen. Intern. Med. 2020, 35, 2801–2803. [Google Scholar] [CrossRef] [PubMed]
- Neill, A.M.; Martin, I.R.; Weir, R.; Anderson, R.; Chereshsky, A.; Epton, M.J.; Jackson, R.; Schousboe, M.; Frampton, C.; Hutton, S.; et al. Community Acquired Pneumonia: Aetiology and Usefulness of Severity Criteria on Admission. Thorax 1996, 51, 1010–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, B.E.; Jones, J.; Bewick, T.; Lim, W.S.; Aronsky, D.; Brown, S.M.; Boersma, W.G.; van der Eerden, M.M.; Dean, N.C. CURB-65 Pneumonia Severity Assessment Adapted for Electronic Decision Support. Chest 2011, 140, 156–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, Y.; Corre, F.; Honsel, V.; Curac, S.; Zarrouk, V.; Fantin, B.; Galy, A. Applicability of the CURB-65 Pneumonia Severity Score for Outpatient Treatment of COVID-19. J. Infect. 2020, 81, e96–e98. [Google Scholar] [CrossRef]
- Satici, C.; Demirkol, M.A.; Sargin Altunok, E.; Gursoy, B.; Alkan, M.; Kamat, S.; Demirok, B.; Surmeli, C.D.; Calik, M.; Cavus, Z.; et al. Performance of Pneumonia Severity Index and CURB-65 in Predicting 30-Day Mortality in Patients with COVID-19. Int. J. Infect. Dis. 2020, 98, 84–89. [Google Scholar] [CrossRef]
- Greco, S.; Salatiello, A.; Fabbri, N.; Passaro, A. Early Prediction of COVID-19 Outcome: Contrasting Clinical Scores and Computational Intelligence Methods. In Studies in Computational Intelligence; Springer: Cham, Switzerland, 2022; Volume 963, pp. 403–423. [Google Scholar]
- Yuan, Y.; Sun, C.; Tang, X.; Cheng, C.; Mombaerts, L.; Wang, M.; Hu, T.; Sun, C.; Guo, Y.; Li, X.; et al. Development and Validation of a Prognostic Risk Score System for COVID-19 Inpatients: A Multi-Center Retrospective Study in China. Engineering 2020, 8, 116–121. [Google Scholar] [CrossRef]
- Knight, S.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.; Dunning, J.; Fairfield, C.; Gamble, C.; Green, C.; et al. Risk Stratification of Patients Admitted to Hospital with Covid-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. Br. Med. J. 2020, 370, m3339. [Google Scholar] [CrossRef]
- Yang, F.; Ma, D. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic. Ann. Intern. Med. 2021, 174, 1343–1344. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Metz, C.E. Basic Principles of ROC Analysis. Semin. Nucl. Med. 1978, 8, 283–298. [Google Scholar] [CrossRef]
- Cortes, C.; Vapnik, V. Support-Vector Networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-Sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Fonti, V.; Belitser, E. Feature Selection Using LASSO; VU Amsterdam: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Tibshirani, R. Regression Shrinkage and Selection Via the Lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Byrd, R.H.; Lu, P.; Nocedal, J.; Zhu, C. A Limited Memory Algorithm for Bound Constrained Optimization. SIAM J. Sci. Comput. 1995, 16, 1190–1208. [Google Scholar] [CrossRef]
- Le, Q.; Sarlós, T.; Smola, A. Fastfood—Approximating Kernel Expansions in Loglinear Time. In Proceedings of the 30th International Conference on Machine Learning, ICML, Atlanta, GA, USA, 16 June–21 June 2013; pp. 1281–1289. [Google Scholar]
- Fawcett, T. An Introduction to ROC Analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Feurer, M.; Hutter, F. Hyperparameter Optimization. In Automated Machine Learning; The Springer Series on Challenges in Machine Learning; Hutter, F., Kotthoff, L., Vanschoren, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–33. [Google Scholar]
- Snoek, J.; Larochelle, H.; Adams, R.P. Practical Bayesian Optimization of Machine Learning Algorithms. In Advances in Neural Information Processing Systems; Curran Associates, Inc.: Red Hook, NY, USA, 2012; Volume 4, pp. 2951–2959. [Google Scholar]
- Wei, P.; Lu, Z.; Song, J. Variable Importance Analysis: A Comprehensive Review. Reliab. Eng. Syst. Saf. 2015, 142, 399–432. [Google Scholar] [CrossRef]
- Fisher, A.; Rudin, C.; Dominici, F. All Models Are Wrong, but Many Are Useful: Learning a Variable’s Importance by Studying an Entire Class of Prediction Models Simultaneously. J. Mach. Learn. Res. 2019, 20, 1–81. [Google Scholar]
- Varol, Y.; Hakoglu, B.; Kadri Cirak, A.; Polat, G.; Komurcuoglu, B.; Akkol, B.; Atasoy, C.; Bayramic, E.; Balci, G.; Ataman, S.; et al. The Impact of Charlson Comorbidity Index on Mortality from SARS-CoV-2 Virus Infection and A Novel COVID-19 Mortality Index: CoLACD. Int. J. Clin. Pract. 2021, 75, e13858. [Google Scholar] [CrossRef]
- Munera, N.; Garcia-Gallo, E.; Gonzalez, Á.; Zea, J.; Fuentes, Y.V.; Serrano, C.; Ruiz-Cuartas, A.; Rodriguez, A.; Reyes, L.F. A Novel Model to Predict Severe COVID-19 and Mortality Using an Artificial Intelligence Algorithm to Interpret Chest Radiographs and Clinical Variables. ERJ Open Res. 2022, 8, 00010–02022. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male Sex Identified by Global COVID-19 Meta-Analysis as a Risk Factor for Death and ITU Admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Zinellu, A.; De Vito, A.; Scano, V.; Paliogiannis, P.; Fiore, V.; Madeddu, G.; Maida, I.; Zinellu, E.; Mangoni, A.A.; Arru, L.B.; et al. The The PaO2/FiO2 Ratio on Admission Is Independently Associated with Prolonged Hospitalization in COVID-19 Patients. J. Infect. Dev. Ctries. 2021, 15, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Kermali, M.; Khalsa, R.K.; Pillai, K.; Ismail, Z.; Harky, A. The Role of Biomarkers in Diagnosis of COVID-19—A Systematic Review. Life Sci. 2020, 254, 117788. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Laboratory Abnormalities in Patients with COVID-2019 Infection. Clin. Chem. Lab. Med. 2020, 58, 1131–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Nam, B.-H.; Kim, M.; Hwang, J.; Kim, J.Y.; Hyun, M.; Kim, H.A.; Cho, C.-H. A Risk Scoring System to Predict Progression to Severe Pneumonia in Patients with Covid-19. Sci. Rep. 2022, 12, 5390. [Google Scholar] [CrossRef]
- Salje, H.; Kiem, C.T.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; Hozé, N.; Richet, J.; Dubost, C.L.; et al. Estimating the Burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA-J. Am. Med. Assoc. 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- McMichael, T.M.; Currie, D.W.; Clark, S.; Pogosjans, S.; Kay, M.; Schwartz, N.G.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; et al. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington. N. Engl. J. Med. 2020, 382, 2005–2011. [Google Scholar] [CrossRef]
- Lanzani, C.; Simonini, M.; Arcidiacono, T.; Messaggio, E.; Bucci, R.; Betti, P.; Avino, M.; Magni, G.; Maggioni, C.; Conte, C.; et al. Role of Blood Pressure Dysregulation on Kidney and Mortality Outcomes in COVID-19. Kidney, Blood Pressure and Mortality in SARS-CoV-2 Infection. J. Nephrol. 2021, 34, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Patanavanich, R.; Glantz, S.A. Smoking Is Associated with COVID-19 Progression: A Meta-Analysis. Nicotine Tob. Res. 2020, 22, 1653–1656. [Google Scholar] [CrossRef]
- Ejaz, H.; Alsrhani, A.; Zafar, A.; Javed, H.; Junaid, K.; Abdalla, A.E.; Abosalif, K.O.A.; Ahmed, Z.; Younas, S. COVID-19 and Comorbidities: Deleterious Impact on Infected Patients. J. Infect. Public Health 2020, 13, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.S.; Sehayek, D.; Gabrielli, S.; Zhang, X.; McCusker, C.; Ben-Shoshan, M. COVID-19 and Comorbidities: A Systematic Review and Meta-Analysis. Postgrad. Med. 2020, 132, 749–755. [Google Scholar] [CrossRef]
- De Giorgi, A.; Fabbian, F.; Greco, S.; Di Simone, E.; De Giorgio, R.; Passaro, A.; Zuliani, G.; Manfredini, R. Prediction of In-Hospital Mortality of Patients with SARS-CoV-2 Infection by Comorbidity Indexes: An Italian Internal Medicine Single Center Study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 10258–10266. [Google Scholar] [CrossRef] [PubMed]
- Tuncer, G.; Surme, S.; Bayramlar, O.F.; Karanalbant, H.K.; Copur, B.; Yazla, M.; Zerdali, E.; Nakir, I.Y.; Cinar, A.R.K.; Buyukyazgan, A.; et al. National Early Warning Score 2 and Laboratory Predictors Correlate with Clinical Deterioration in Hospitalized Patients with COVID-19. Biomark. Med. 2021, 15, 807–820. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081. [Google Scholar] [CrossRef]
- Zhao, Z.; Chen, A.; Hou, W.; Graham, J.M.; Li, H.; Richman, P.S.; Thode, H.C.; Singer, A.J.; Duong, T.Q. Prediction Model and Risk Scores of ICU Admission and Mortality in COVID-19. PLoS ONE 2020, 15, e0236618. [Google Scholar] [CrossRef] [PubMed]
- López-Escobar, A.; Madurga, R.; Castellano, J.M.; Velázquez, S.; Suárez Del Villar, R.; Menéndez, J.; Peixoto, A.; Jimeno, S.; Ventura, P.S.; Ruiz de Aguiar, S. Risk Score for Predicting In-Hospital Mortality in COVID-19 (Rim Score). Diagnostics 2021, 11, 596. [Google Scholar] [CrossRef] [PubMed]
- Halasz, G.; Sperti, M.; Villani, M.; Michelucci, U.; Agostoni, P.; Biagi, A.; Rossi, L.; Botti, A.; Mari, C.; Maccarini, M.; et al. A Machine Learning Approach for Mortality Prediction in COVID-19 Pneumonia: Development and Evaluation of the Piacenza Score. J. Med. Internet Res. 2021, 23, e29058. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, S.; Cacia, M.; Leo, I.; Polimeni, A.; Sabatino, J.; Spaccarotella, C.A.M.; Mongiardo, A.; De Rosa, S.; Indolfi, C. B-Type Natriuretic Peptide as Biomarker of COVID-19 Disease Severity—A Meta-Analysis. J. Clin. Med. 2020, 9, 2957. [Google Scholar] [CrossRef] [PubMed]
- Soni, M.; Gopalakrishnan, R.; Vaishya, R.; Prabu, P. D-Dimer Level Is a Useful Predictor for Mortality in Patients with COVID-19: Analysis of 483 Cases. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2245–2249. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cohort Characteristics | All Patients (N = 250) | IoCp (N = 76) | NIoCp (N = 174) | p-Value | Deceased (N = 62) | Discharged (N = 188) | p-Value | 30-ddp (N = 59) | 30-dsp (N = 191) | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| Males, n (%) | 137 (54.8) | 50 (65.8) | 87 (50.0) | 0.021 | 31 (50.0) | 106 (56.4) | 0.38 | 31 (52.5) | 109 (57.1) | 0.20 |
| Females, n (%) | 113 (45.2) | 26 (34.2) | 87 (50.0) | 31 (50.0) | 82 (43.6) | 28 (47.5) | 82 (42.9) | |||
| Age, years | 72 (58–82) | 72 (62–80) | 72 (53–82) | 0.26 | 82 (76–86) | 67 (53–78) | <0.001 | 81 (73–86) | 68 (54–79) | <0.001 |
| Length of stay, days | 12 (7–22) | 21 (12–40) | 10 (6–16) | <0.001 | 10 (6–20) | 12 (7–23) | 0.16 | 9 (6–16) | 13 (8–24) | <0.001 |
| GASS score, points | 7 (5–11) | 9 (7–11) | 7 (4–10) | <0.001 | 11 (9–13) | 6 (4–9) | <0.001 | 11 (8–13) | 7 (4–9) | <0.001 |
| CCI, points ± SD | 2.0 ± 2.5 | 2.1 ± 2.5 | 2.0 ± 2.5 | 0.69 | 3.3 ± 2.7 | 1.6 ± 2.3 | <0.001 | 3.0 ± 2.6 | 1.7 ± 2.4 | 0.001 |
| Vital Signs and Parameters | ||||||||||
| SBP, mmHg | 130 (120–140) | 130 (120–150) | 130 (115–140) | 0.47 | 120 (110–140) | 130 (120–140) | 0.024 | 120 (110–130) | 130 (120–140) | 0.005 |
| DBP, mmHg | 70 (70–80) | 70 (60–80) | 70 (70–80) | 0.08 | 70 (60–80) | 75 (70–80) | 0.019 | 70 (60–80) | 75 (70–80) | 0.003 |
| HR, bpm | 86 (77–99) | 86 (75–100) | 87 (78–99) | 0.39 | 88 (76–100) | 86 (78–99) | 0.94 | 88 (74–100) | 86 (78–99) | 0.84 |
| RR, apm | 20 (18–23) | 22 (20–30) | 20 (16–22) | <0.001 | 22 (18–28) | 20 (16–22) | <0.001 | 21 (18–28) | 20 (16–22) | 0.016 |
| PaO2/FiO2 ratio | 300 (230–352) | 229 (155–295) | 310 (261–355) | <0.001 | 266 (200–304) | 310 (244–355) | 0.09 | 269 (193–311) | 308 (245–352) | 0.22 |
| Laboratory Findings | ||||||||||
| WBC (n/mmc) | 6395 (4815–9375) | 6970 (5315–9795) | 6210 (4750–9280) | 0.33 | 7600 (5380–10905) | 6140 (4750–9010) | 0.07 | 6280 (5060–10030) | 6420 (4795–9320) | 0.84 |
| Lymphocytes (n/mmc) | 1000 (740–1390) | 990 (635–1325) | 1000 (760–1470) | 0.33 | 870 (640–1085) | 1050 (778–1483) | 0.008 | 905 (658–1278) | 1030 (770–1465) | 0.14 |
| Creatinine (mg/dl) | 0.94 (0.77–1.28) | 0.96 (0.78–1.35) | 0.94 (0.77–1.24) | 0.78 | 1.34 (0.82–2.01) | 0.91 (0.75–1.16) | <0.001 | 1.31 (0.88–1.83) | 0.91 (0.75–1.17) | <0.001 |
| CRP (mg/dl) | 5.82 (1.98–10.92) | 8.57 (1.94–18.00) | 5.21 (1.98–9.52) | 0.038 | 8.49 (3.10–13.71) | 4.92 (1.74–9.87) | 0.007 | 8.49 (2.87–12.88) | 4.98 (1.83–10.12) | 0.025 |
| Procalcitonin (ng/mL) | 0.15 (0.05–0.51) | 0.25 (0.08–0.73) | 0.11 (0.05–0.43) | 0.018 | 0.54 (0.20–1.75) | 0.09 (0.05–0.26) | <0.001 | 0.49 (0.17–1.96) | 0.10 (0.05–0.27) | <0.001 |
| Fibrinogen (mg/dl) | 509 (441–659) | 555 (438–689) | 501 (441–643) | 0.27 | 572 (431–677) | 502 (441–642) | 0.37 | 550 (428–674) | 506 (441–643) | 0.91 |
| D-Dimer (mg/L FEU) | 0.93 (0.54–2.04) | 1.12 (0.74–1.99) | 0.88 (0.47–2.04) | 0.039 | 1.20 (0.77–2.30) | 0.85 (0.47–1.80) | 0.008 | 1.15 (0.76–2.00) | 0.88 (0.48–2.04) | 0.044 |
| Isoamylase (U/L) | 27 (20–44) | 36 (25–100) | 26 (18–41) | 0.008 | 32 (18–51) | 27 (21–44) | 0.92 | 36 (20–45) | 27 (20–43) | 0.63 |
| ALT (U/L) | 21 (14–37) | 26 (18–49) | 19 (12–33) | 0.003 | 18 (11–29) | 87 (52–193) | 0.06 | 19 (12–34) | 21 (14–37) | 0.29 |
| CPK (U/L) | 87 (51–203) | 111 (54–224) | 83 (46–169) | 0.14 | 93 (50–220) | 280 (211–361) | 0.82 | 122 (59–356) | 86 (50–167) | 0.12 |
| LDH (U/L) | 286 (219–380) | 390 (274–466) | 271 (210–332) | <0.001 | 328 (250–436) | 304 (125–593) | 0.015 | 332 (265–434) | 276 (210–358) | 0.001 |
| Ferritin (ng/mL) | 327 (142–637) | 506 (294–922) | 275 (120–565) | 0.006 | 364 (180–767) | 304 (125–593) | 0.19 | 439 (264–736) | 293 (121–610) | 0.07 |
| BNP (pg/mL) | 76 (36–185) | 80 (43–168) | 75 (33–195) | 0.90 | 197 (94–410) | 60 (30–126) | <0.001 | 209 (87–377) | 62 (30–132) | <0.001 |
| HS TnI (ng/mL) | 14 (5–34) | 15 (7–47) | 13 (5–29) | 0.13 | 41 (16–85) | 9 (4–21) | <0.001 | 42 (19–101) | 9 (4–22) | <0.001 |
| Comorbidity | All Patients (N = 250) | IoCp (N = 76) | NIoCp (N = 174) | p-Value | Deceased (N = 62) | Discharged (N = 188) | p-Value | 30-ddp (N = 59) | 30-dsp (N = 191) | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| Smoking habit | 53 (21.2) | 25 (32.9) | 28 (16.1) | 0.003 | 17 (27.4) | 36 (19.1) | 0.17 | 14 (23.7) | 39 (20.4) | 0.59 |
| Hypertension | 141 (56.4) | 49 (64.5) | 92 (52.9) | 0.09 | 45 (72.6) | 96 (51.1) | 0.003 | 45 (76.3) | 96 (50.3) | <0.001 |
| Ischemic heart disease | 25 (10.0) | 8 (10.5) | 17 (9.8) | 0.86 | 11 (17.7) | 14 (7.4) | 0.019 | 9 (15.3) | 16 (8.4) | 0.12 |
| Heart failure | 18 (7.2) | 5 (6.6) | 13 (7.5) | 0.80 | 8 (12.9) | 10 (5.3) | 0.045 | 6 (10.2) | 12 (6.3) | 0.31 |
| Chronic kidney disease (moderate or severe) | 35 (14.0) | 10 (13.2) | 25 (14.4) | 0.80 | 15 (24.2) | 20 (10.6) | 0.008 | 13 (22.0) | 22 (11.5) | 0.042 |
| Stroke or TIA | 33 (13.2) | 8 (10.5) | 25 (14.4) | 0.41 | 17 (27.4) | 16 (8.5) | <0.001 | 15 (25.4) | 18 (9.4) | 0.002 |
| PAD | 16 (6.4) | 3 (3.9) | 13 (7.5) | 0.30 | 9 (14.5) | 7 (3.7) | 0.003 | 8 (13.6) | 8 (4.2) | 0.010 |
| COPD | 26 (10.4) | 9 (11.8) | 17 (9.8) | 0.62 | 13 (21.0) | 13 (6.9) | 0.002 | 10 (16.9) | 16 (8.4) | 0.06 |
| Mild hepatopathy | 8 (3.2) | 0 (0) | 8 (4.6) | 0.06 | 1 (1.6) | 7 (3.7) | 0.41 | 1 (1.7) | 7 (3.7) | 0.45 |
| Moderate or severe hepatopathy | 3 (1.2) | 1 (1.3) | 2 (1.1) | 0.91 | 3 (4.8) | 0 (0) | 0.002 | 3 (5.1) | 0 (0) | 0.002 |
| Localized or hematological cancer | 49 (19.6) | 17 (22.4) | 32 (18.4) | 0.47 | 19 (30.6) | 30 (15.9) | 0.012 | 19 (32.2) | 30 (15.7) | 0.005 |
| Metastatic cancer | 11 (4.4) | 3 (3.9) | 8 (4.6) | 0.82 | 2 (3.2) | 9 (4.8) | 0.60 | 1 (1.7) | 10 (5.2) | 0.25 |
| Dementia | 47 (18.8) | 13 (17.1) | 34 (19.5) | 0.65 | 22 (35.5) | 25 (13.3) | <0.001 | 20 (33.8) | 27 (14.1) | 0.001 |
| Diabetes without organ damage | 23 (9.2) | 7 (9.2) | 16 (9.2) | 1.00 | 7 (11.3) | 16 (8.5) | 0.51 | 8 (13.6) | 15 (7.9) | 0.19 |
| Diabetes with organ damage | 26 (10.4) | 9 (11.8) | 17 (9.8) | 0.62 | 11 (17.7) | 15 (8.0) | 0.029 | 9 (15.3) | 17 (8.9) | 0.16 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
|
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, S.; Salatiello, A.; Fabbri, N.; Riguzzi, F.; Locorotondo, E.; Spaggiari, R.; De Giorgi, A.; Passaro, A. Rapid Assessment of COVID-19 Mortality Risk with GASS Classifiers. Biomedicines 2023, 11, 831. https://doi.org/10.3390/biomedicines11030831
Greco S, Salatiello A, Fabbri N, Riguzzi F, Locorotondo E, Spaggiari R, De Giorgi A, Passaro A. Rapid Assessment of COVID-19 Mortality Risk with GASS Classifiers. Biomedicines. 2023; 11(3):831. https://doi.org/10.3390/biomedicines11030831
Chicago/Turabian StyleGreco, Salvatore, Alessandro Salatiello, Nicolò Fabbri, Fabrizio Riguzzi, Emanuele Locorotondo, Riccardo Spaggiari, Alfredo De Giorgi, and Angelina Passaro. 2023. "Rapid Assessment of COVID-19 Mortality Risk with GASS Classifiers" Biomedicines 11, no. 3: 831. https://doi.org/10.3390/biomedicines11030831