





Abstract
Background: Women consistently have higher sickness absence than men. The double-burden hypothesis suggests this is due to higher work–family burden in women than men. The current study aimed to systematically review prospective studies of work–family conflict and subsequent sickness absence. Methods: A systematic search was conducted in the electronic databases Medline, PsycINFO, and Embase with subject heading terms and keywords with no language or time restrictions. Two reviewers independently screened abstracts and read full-texts with pre-defined inclusion and exclusion criteria. Results: Eight included studies (n = 40 856 respondents) measure perceived work–family conflict and subsequent sickness absence. We found moderate evidence for a positive relationship between work–family conflict and subsequent sickness absence, and that women experience higher levels of work–family conflict than men. Conclusion: Work–family conflict is associated with later sickness absence, and work–family conflict is more common for women than for men. This indicates that work–family conflict may contribute to the gender gap in sick leave. However, further studies are needed to confirm whether this relationship is causal.
Introduction
Sickness absence represents a financial burden to organizations and the society at large, and is also a gateway to long-term disability and labour market exclusion.1 Several studies have examined the importance of work and health predictors of sickness absence; such as occupational factors (e.g. job demands and resources), lifestyle and health behaviours (e.g. obesity, physical health and smoking) and mental health factors.2,3 The increase of both dual-earner families and single parents in the work force advocate a focus on the conflict between work and family to fully understand the aetiology of sickness absence.
Women have higher sickness absence rates than men in most western countries,3–7 with an increase in several countries over the past decades.6 However, the mechanisms of the gender gap in sickness absence are still not fully understood. The proposed mechanisms, such as biological (e.g. pregnancy related illness, increases in maternal age at birth),8 work- and educational (e.g. occupation, education level and work demands)9 and health-related mechanisms (e.g. somatic and mental health),9 cannot fully explain the gender gap. For instance, one finding reported that even when adjusting for a range of factors such as occupation, working conditions, somatic and mental health, this could only account for a modest portion of the gender differences in sickness absence.9 Studies have also yielded some unexpected findings, such as younger mothers having a higher risk for sickness absence compared with older mothers, despite older birth age being a risk factor for birth complications.8 The double burden hypothesis has been suggested as an explanation for the gender gap in sickness absence.10,11
‘The double burden hypothesis’ is embedded in ‘the role strain theory’ suggesting that the combination of multiple roles, such as being an employee and a parent, increase work strain and adverse health outcomes.4,10,12 This in turn might increase the risk for sickness absence.2,3,10 Despite some changes in household patterns over the past decades, women still spend more time and have the primary responsibility for household tasks and childcare compared to men.13 Also, in line with traditional gender role orientations and expectations, women report more problems and negative effects with these domestic stressors.13 Still, the empirical support for the double burden hypothesis is ambiguous.4,10 With the exception of a few studies in which parenthood predict higher levels of sickness absence,5,10,11 other studies do not support the double burden.3,4,14 In a study covering 24 European countries, Mastekaasa15 reported that among women with partners, having children was in fact associated with lower sickness absence. This does not give support to the double burden/role strain theory, but rather supports a competing theory called the role accumulation theory arguing that multiple roles can outweigh the strains experienced, possibly through a protective effect of social support or positive self-image from different contexts.16 It may also be caused by selection, if healthier women more often have children. However, the majority of these studies have counted number of children or role memberships (e.g. occupational, parental and civil status), which despite of their objectivity might be an unsatisfying proxy for capturing the complexity of the perceived conflict or demands experienced when having multiple roles. Mastekaasa15 reported some tendencies for mothers with a single small child (ages 0–5) to have higher sickness absence indicating that it is the transition to parenthood and the related new demands which is associated with higher sickness absence. This suggests moving beyond counting children or role memberships, to capture the complexity of the double burden that might be experienced when combining family and work.
Measuring experienced family stressors, such as perceived work–family conflict, might better reflect the burden of having multiple roles and thus predict adverse consequences such as sickness absence. For non-parents, work–family conflict could capture the effect of double burden from family demands that are not related to having children, a perspective that is lacking in studies counting number of children or role memberships. Work–family conflict is linked to formerly reported predictors of sickness absence,2,3 like higher levels of job dissatisfaction, burnout, and health problems.17–22 Earlier reviews of cross-sectional studies report that work–family conflict and sickness absence are associated,18,23 but the studies are vulnerable to methodological problems like reverse causation and self-serving attribution bias. There is a thus a need for an updated systematic review focusing on longitudinal studies.
Work–family conflict is defined by ‘interrole conflict in which the role pressures from work and family domains are mutually incompatible’,24 when time, strain and specific behaviours required in one role interferes with fulfilling the other role. Work–family conflict can have different directions: Work demands can interfere with the family role (i.e. ‘work-to-family conflict’), or family demands can interfere with the work role (i.e. ‘family-to-work conflict’).23–25 Findings from meta-analyses and systematic reviews indicate low correlations, different consequences and prevalence for work-to-family and family-to-work conflict, which suggest that there are sufficient enough unique variance for separate examination.18,22,25,26 Work-to-family conflict appears to be more strongly associated with work-related factors than family-to work conflict.18,22,26 These two concepts are thus treated separately in the current review.
Some findings indicate gender differences in prevalence, predictors and consequences of work–family conflict.23 Despite some ambiguous findings of gender differences in work–family conflict levels; there is a tendency for women to report higher levels than men—with stronger effects in samples of parents.19,23,26
H1: Perceived work–family conflict is prospectively associated with higher sickness absence (path b in figure 1).
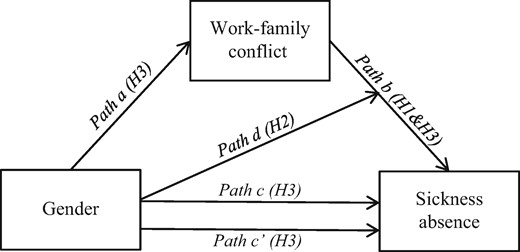
Conceptual figure illustrating the proposed model guiding the systematic review of the longitudinal association between work-family conflict and sickness absence. H1, Hypothesis 1; H2, Hypothesis 2; H3, Hypothesis 3
If this hypothesis is supported, studying work–family conflict might be a better way to examine the double burden hypothesis than counting children or role membership.
H2: The prospective association between work-family conflict and sickness absence is moderated by gender—i.e, the association is stronger for women than for men (path d in figure 1).
If this hypothesis is supported, this yields support for the double burden hypothesis for the gender gap in sickness absence—in which women are more vulnerable for sickness absence when perceiving work–family conflict.
H3: The association between gender and sickness absence is partly mediated by work-family conflict (path c and c' in figure 1).
For mediation to occur, an appropriate criterion for mediation must have been used. For instance the causal-step approach by Baron and Kenny (1986), the Sobel-test or indirect path analyses with structural equation modelling. With the causal-step approach four assumptions should be met for mediation to occur (see figure 1): (i) Gender (the predictor) significantly predicts sickness absence (the outcome) at follow-up before adjusting for work–family conflict (the mediator) at baseline (path c in figure 1); (ii) Gender significantly predicts work–family conflict (path a); (iii) Work–family conflict at baseline significantly predicts sickness absence at follow-up (paths b); and (iv) The significant association between gender and sickness absence (the path c’) is either eliminated (in case of total mediation) or reduced significantly (in case of partial mediation) when work–family conflict (the mediator) is adjusted for. If this hypothesis is supported, this supports for the double burden hypothesis for the gender gap in sickness absence—in which this gap can be explained by women having higher levels of perceived work–family conflict.
Methods
Search and screening strategy
Three steps were used to identify studies. First, a systematic literature search was conducted with the electronic databases Medline, PsycINFO and Embase using medical subject heading terms and key words in February 2014. We used three comprehensive clusters of keywords and subject headings related to (i) the exposure (e.g. ‘home’, ‘family’ and ‘parenthood’), (ii) the outcome (e.g. ‘sickness absence’, ‘sick leave’ and ‘absenteeism’), (iii) study design (e.g. ‘longitudinal’ and ‘follow-up’). The search was not limited to years or language. We searched Google/Google Scholar and inspected references list of relevant article to identify further relevant articles. A new search was conducted in April 2016 where ‘work–family conflict’ and similar concepts was used as the exposure cluster of search terms. See Supplementary Material for the search strategy.
Second, two authors screened the abstracts independently for quantitative prospective studies examining work–family conflict or similar terms (e.g. work–family/home/non-work conflict/interference/spill-over) and sickness absence. When disagreement occurred, a third author was involved.
Third, relevant full-texts were retrieved and read. Studies were included when meeting all the following criteria: (i) study design: ≥2 measuring point, (ii) sample: healthy, working individuals, (iii) relevant measures of perceived work–family conflict (or related concept) and sickness absence and (iv) statistical test of the prospective association between work–family conflict and sickness absence. Quality assessments of study design, exposures and outcomes were conducted by two authors independently with the following predefined criteria of quality with a focus on possible risks of bias and generalizability: (i) Follow-up period >6 months); (ii) Sample > 400 and (iii) Response rate (>70%); (iv) Reliable and/or valid exposure variable (Cronbach alpha > 0.70 and/or face validity); (v) Reliable and/or valid outcome variable (Cronbach alpha > 0.70 and/or face validity); (vi) Risk of common method bias; and (vii) Adjustment of >3 essential confounders (age, education, partner status, children, health- or work factors).
Evidence synthesis
The top part of the fraction indicates the number of positive relationships, subtracting the negative relationships, while the bottom part represents the total number of included studies (including those with non-significant relationships). Thus, SIC ranges from −1, representing all available studies showing negative relationships), to +1, representing only positive relationships, and 0, representing either inconsistent or insignificant findings. SIC is thus a measure of consistent findings. We follow Wielenga-Meijer, Taris27 recommendations to combine the consistency of the relationships (e.g. SIC-scores) and the number of studies, resulting in eight categories of strength of the evidence: (i) Strong evidence, (ii) Moderate evidence, (iii) Limited evidence and (iv) Inconsistent evidence (i.e. ambivalent findings, null findings, or insufficient evidence (less than two studies). See Supplementary Material for more detail.
Results
The initial 2014 search revealed 2260 titles after removing duplicates. In total, 179 titles matched the inclusion criteria and were read in full text. Seven studies met the criteria of examining prospective associations between family-related stressors and sickness absence after reading full text articles.29–35 See Supplementary Material for the full PRISMA flow chart. The search in 2016 revealed additional 125 titles, of which one new study36 was included, resulting in eight included studies in total.
All studies were published in English between 2005 and 2015. The studies were from the Netherlands (n = 1),33 Sweden (n = 3),29,30,34 Finland (n = 1),35 Belgium (n = 2)31,32 and Norway (n = 1).36 The study design was longitudinal studies with follow-up time varying from six months to three years measuring work–family conflict at baseline and sickness absence at follow-up. Sample sizes ranged from 1583 to 18 366. All studies restricted their samples to employees. Two studies only including women29,28 were based on the same study. Four studies conducted all analyses separately for men and women,32–35 and two combined men and women in all analyses.31,36 The samples ranged from 23 to 70% in having children (using varying definitions of ages) and 60–100% of the participants in the samples having a partner. See table 1 for study design and instrument description.
Study characteristics and operationalization of work–family conflict and sickness absence
| Study | Study design, population, follow-up duration | Exposure variable | Outcome variable |
|---|---|---|---|
| Casini et al. (2013) | 3465 Belgian women and men aged 21–66; 1-year follow-up | ‘Work-to-home conflict’ (five items) at baseline: The “Inability to withdraw from work ‘-subscale’37; mean score; Cronbach alpha > 0.80; ‘Home-to-work conflict’ (six items) at baseline: The ‘Home-work interference scale’25; mean scores; Cronbach alpha = 0.54 | Medically certified sickness absence from employers’ registries during 12 months from baseline, excluding chronic illness and maternity leave. ‘Frequency’: total number of episodes; ‘Duration’: total number of days. |
| Clays et al. (2009) | 2983 Belgian women and men aged 30–55; 1-year follow-up | ‘Work-to-home conflict’ (six items) at baseline: Based on scale by Kelloway et al.25; Sum score; Cronbach alpha>0.80; ‘Home-to-work conflict’ (six items) at baseline: Missing information on origin; sum score; Cronbach alpha > 0.80 | Medically certified sickness absence from employers’ registries during 12 months from baseline. ‘Frequency’: Three or more episodes; ‘Duration’: Ten or more days. |
| Jansen et al. (2006) | 3789 Dutch women and men with mean ages 39.89 (SD:8.75)–44.74 (SD:8.20); 6 months follow-up | ‘Work-to-home’ (six items) and ‘home-to-work conflict’ (five items) at baseline: Shortened version of Survey Work-Home Interference Nijmegen20; Sum scores dichotomized in high vs. low/medium; Missing reliability; ‘General work–family conflict’ (11 items) at baseline: Sum score of all items dichotomized into high vs. low-medium; Missing reliability | ‘Duration’ of new sickness absence-incidences from employers’ registries 6 months from baseline. Pregnant women and employees on sick leave at baseline were excluded. |
| Lidwall et al. (2009) | 2867 Swedish women and men aged 25–50; 1-year follow-up | ‘Work-to-family’ (one item) and ‘family-to-work conflict’ (one item) at baseline: Scale from The General Nordic Questionnaire for Psychological and Social Factors at Work (QPS-Nordic)38; dichotomized into no conflict or more than some time during the week; Missing reliability | ‘Duration’ of medically certified long-term continuous sickness absence-period of at least 14 days from national social insurance registries. Participants were excluded if they were on disability pension at baseline. |
| Roelen et al. (2015) | 1557 Norwegian women (91%) and men with mean age 33.1 (SD:8.2); 1- and 2-year follow-ups | ‘Work-to-family’ (four items) and ‘family-to-work conflict’ (four items) at baseline and first follow-up: The Work–Family interface scale1; mean score; Cronbach alpha = 0.80 and 0.77. | ‘Duration’ of self-reported absence the last 12 months due to illness or injury at waves. High sickness absence was defined as > 30 days the past 12 months. Care-related sick leave for children or family members was excluded. |
| Vaananen et al. (2008) | 18366 Finnish women and men aged 20–64; 17 month (on average) follow-up | ‘Negative work-to-family spillover’ (three items) at baseline: Scale by Maardberg et al.39; Sum score categorized to three categories (high, moderate, low); Cronbach alphas > 0.80 | ‘Frequency’ of sickness absence from employers’ registries of more than 3 days during the follow-up computed as the number of absences per 100 and 1000 employee a year. |
| Vingård et al. (2005) | 6246 Swedish women up to age 61; 3-year follow-up | ‘General work–family conflict’ (two items) at baseline: One item each on work to family, and family to work conflict; Missing information on origin, use and reliability | ‘Frequency’ of employers-reported new spells of 28 or more days of consecutively sickness absence 3 years from baseline. |
| Voss et al. (2008) | 1583 Swedish women under age 50; 1-year follow-up | ‘General work–family conflict’ (two items) at baseline: Work negatively affecting home; and vice versa; Information on origin refers to the included study by Vingård et al.29 Dichotomized to the presence of work–family conflict when replying very often or always to at least one of the two items. | ‘Frequency’ of employer registered new sickness absence-spells during 2001 with (i) the number of subjects with four or more new sickness absence spells and (ii) long-term sickness absence with all spells longer than 28 days. |
| Study | Study design, population, follow-up duration | Exposure variable | Outcome variable |
|---|---|---|---|
| Casini et al. (2013) | 3465 Belgian women and men aged 21–66; 1-year follow-up | ‘Work-to-home conflict’ (five items) at baseline: The “Inability to withdraw from work ‘-subscale’37; mean score; Cronbach alpha > 0.80; ‘Home-to-work conflict’ (six items) at baseline: The ‘Home-work interference scale’25; mean scores; Cronbach alpha = 0.54 | Medically certified sickness absence from employers’ registries during 12 months from baseline, excluding chronic illness and maternity leave. ‘Frequency’: total number of episodes; ‘Duration’: total number of days. |
| Clays et al. (2009) | 2983 Belgian women and men aged 30–55; 1-year follow-up | ‘Work-to-home conflict’ (six items) at baseline: Based on scale by Kelloway et al.25; Sum score; Cronbach alpha>0.80; ‘Home-to-work conflict’ (six items) at baseline: Missing information on origin; sum score; Cronbach alpha > 0.80 | Medically certified sickness absence from employers’ registries during 12 months from baseline. ‘Frequency’: Three or more episodes; ‘Duration’: Ten or more days. |
| Jansen et al. (2006) | 3789 Dutch women and men with mean ages 39.89 (SD:8.75)–44.74 (SD:8.20); 6 months follow-up | ‘Work-to-home’ (six items) and ‘home-to-work conflict’ (five items) at baseline: Shortened version of Survey Work-Home Interference Nijmegen20; Sum scores dichotomized in high vs. low/medium; Missing reliability; ‘General work–family conflict’ (11 items) at baseline: Sum score of all items dichotomized into high vs. low-medium; Missing reliability | ‘Duration’ of new sickness absence-incidences from employers’ registries 6 months from baseline. Pregnant women and employees on sick leave at baseline were excluded. |
| Lidwall et al. (2009) | 2867 Swedish women and men aged 25–50; 1-year follow-up | ‘Work-to-family’ (one item) and ‘family-to-work conflict’ (one item) at baseline: Scale from The General Nordic Questionnaire for Psychological and Social Factors at Work (QPS-Nordic)38; dichotomized into no conflict or more than some time during the week; Missing reliability | ‘Duration’ of medically certified long-term continuous sickness absence-period of at least 14 days from national social insurance registries. Participants were excluded if they were on disability pension at baseline. |
| Roelen et al. (2015) | 1557 Norwegian women (91%) and men with mean age 33.1 (SD:8.2); 1- and 2-year follow-ups | ‘Work-to-family’ (four items) and ‘family-to-work conflict’ (four items) at baseline and first follow-up: The Work–Family interface scale1; mean score; Cronbach alpha = 0.80 and 0.77. | ‘Duration’ of self-reported absence the last 12 months due to illness or injury at waves. High sickness absence was defined as > 30 days the past 12 months. Care-related sick leave for children or family members was excluded. |
| Vaananen et al. (2008) | 18366 Finnish women and men aged 20–64; 17 month (on average) follow-up | ‘Negative work-to-family spillover’ (three items) at baseline: Scale by Maardberg et al.39; Sum score categorized to three categories (high, moderate, low); Cronbach alphas > 0.80 | ‘Frequency’ of sickness absence from employers’ registries of more than 3 days during the follow-up computed as the number of absences per 100 and 1000 employee a year. |
| Vingård et al. (2005) | 6246 Swedish women up to age 61; 3-year follow-up | ‘General work–family conflict’ (two items) at baseline: One item each on work to family, and family to work conflict; Missing information on origin, use and reliability | ‘Frequency’ of employers-reported new spells of 28 or more days of consecutively sickness absence 3 years from baseline. |
| Voss et al. (2008) | 1583 Swedish women under age 50; 1-year follow-up | ‘General work–family conflict’ (two items) at baseline: Work negatively affecting home; and vice versa; Information on origin refers to the included study by Vingård et al.29 Dichotomized to the presence of work–family conflict when replying very often or always to at least one of the two items. | ‘Frequency’ of employer registered new sickness absence-spells during 2001 with (i) the number of subjects with four or more new sickness absence spells and (ii) long-term sickness absence with all spells longer than 28 days. |
Note: References to all scales are included as Supplementary Material.
Study characteristics and operationalization of work–family conflict and sickness absence
| Study | Study design, population, follow-up duration | Exposure variable | Outcome variable |
|---|---|---|---|
| Casini et al. (2013) | 3465 Belgian women and men aged 21–66; 1-year follow-up | ‘Work-to-home conflict’ (five items) at baseline: The “Inability to withdraw from work ‘-subscale’37; mean score; Cronbach alpha > 0.80; ‘Home-to-work conflict’ (six items) at baseline: The ‘Home-work interference scale’25; mean scores; Cronbach alpha = 0.54 | Medically certified sickness absence from employers’ registries during 12 months from baseline, excluding chronic illness and maternity leave. ‘Frequency’: total number of episodes; ‘Duration’: total number of days. |
| Clays et al. (2009) | 2983 Belgian women and men aged 30–55; 1-year follow-up | ‘Work-to-home conflict’ (six items) at baseline: Based on scale by Kelloway et al.25; Sum score; Cronbach alpha>0.80; ‘Home-to-work conflict’ (six items) at baseline: Missing information on origin; sum score; Cronbach alpha > 0.80 | Medically certified sickness absence from employers’ registries during 12 months from baseline. ‘Frequency’: Three or more episodes; ‘Duration’: Ten or more days. |
| Jansen et al. (2006) | 3789 Dutch women and men with mean ages 39.89 (SD:8.75)–44.74 (SD:8.20); 6 months follow-up | ‘Work-to-home’ (six items) and ‘home-to-work conflict’ (five items) at baseline: Shortened version of Survey Work-Home Interference Nijmegen20; Sum scores dichotomized in high vs. low/medium; Missing reliability; ‘General work–family conflict’ (11 items) at baseline: Sum score of all items dichotomized into high vs. low-medium; Missing reliability | ‘Duration’ of new sickness absence-incidences from employers’ registries 6 months from baseline. Pregnant women and employees on sick leave at baseline were excluded. |
| Lidwall et al. (2009) | 2867 Swedish women and men aged 25–50; 1-year follow-up | ‘Work-to-family’ (one item) and ‘family-to-work conflict’ (one item) at baseline: Scale from The General Nordic Questionnaire for Psychological and Social Factors at Work (QPS-Nordic)38; dichotomized into no conflict or more than some time during the week; Missing reliability | ‘Duration’ of medically certified long-term continuous sickness absence-period of at least 14 days from national social insurance registries. Participants were excluded if they were on disability pension at baseline. |
| Roelen et al. (2015) | 1557 Norwegian women (91%) and men with mean age 33.1 (SD:8.2); 1- and 2-year follow-ups | ‘Work-to-family’ (four items) and ‘family-to-work conflict’ (four items) at baseline and first follow-up: The Work–Family interface scale1; mean score; Cronbach alpha = 0.80 and 0.77. | ‘Duration’ of self-reported absence the last 12 months due to illness or injury at waves. High sickness absence was defined as > 30 days the past 12 months. Care-related sick leave for children or family members was excluded. |
| Vaananen et al. (2008) | 18366 Finnish women and men aged 20–64; 17 month (on average) follow-up | ‘Negative work-to-family spillover’ (three items) at baseline: Scale by Maardberg et al.39; Sum score categorized to three categories (high, moderate, low); Cronbach alphas > 0.80 | ‘Frequency’ of sickness absence from employers’ registries of more than 3 days during the follow-up computed as the number of absences per 100 and 1000 employee a year. |
| Vingård et al. (2005) | 6246 Swedish women up to age 61; 3-year follow-up | ‘General work–family conflict’ (two items) at baseline: One item each on work to family, and family to work conflict; Missing information on origin, use and reliability | ‘Frequency’ of employers-reported new spells of 28 or more days of consecutively sickness absence 3 years from baseline. |
| Voss et al. (2008) | 1583 Swedish women under age 50; 1-year follow-up | ‘General work–family conflict’ (two items) at baseline: Work negatively affecting home; and vice versa; Information on origin refers to the included study by Vingård et al.29 Dichotomized to the presence of work–family conflict when replying very often or always to at least one of the two items. | ‘Frequency’ of employer registered new sickness absence-spells during 2001 with (i) the number of subjects with four or more new sickness absence spells and (ii) long-term sickness absence with all spells longer than 28 days. |
| Study | Study design, population, follow-up duration | Exposure variable | Outcome variable |
|---|---|---|---|
| Casini et al. (2013) | 3465 Belgian women and men aged 21–66; 1-year follow-up | ‘Work-to-home conflict’ (five items) at baseline: The “Inability to withdraw from work ‘-subscale’37; mean score; Cronbach alpha > 0.80; ‘Home-to-work conflict’ (six items) at baseline: The ‘Home-work interference scale’25; mean scores; Cronbach alpha = 0.54 | Medically certified sickness absence from employers’ registries during 12 months from baseline, excluding chronic illness and maternity leave. ‘Frequency’: total number of episodes; ‘Duration’: total number of days. |
| Clays et al. (2009) | 2983 Belgian women and men aged 30–55; 1-year follow-up | ‘Work-to-home conflict’ (six items) at baseline: Based on scale by Kelloway et al.25; Sum score; Cronbach alpha>0.80; ‘Home-to-work conflict’ (six items) at baseline: Missing information on origin; sum score; Cronbach alpha > 0.80 | Medically certified sickness absence from employers’ registries during 12 months from baseline. ‘Frequency’: Three or more episodes; ‘Duration’: Ten or more days. |
| Jansen et al. (2006) | 3789 Dutch women and men with mean ages 39.89 (SD:8.75)–44.74 (SD:8.20); 6 months follow-up | ‘Work-to-home’ (six items) and ‘home-to-work conflict’ (five items) at baseline: Shortened version of Survey Work-Home Interference Nijmegen20; Sum scores dichotomized in high vs. low/medium; Missing reliability; ‘General work–family conflict’ (11 items) at baseline: Sum score of all items dichotomized into high vs. low-medium; Missing reliability | ‘Duration’ of new sickness absence-incidences from employers’ registries 6 months from baseline. Pregnant women and employees on sick leave at baseline were excluded. |
| Lidwall et al. (2009) | 2867 Swedish women and men aged 25–50; 1-year follow-up | ‘Work-to-family’ (one item) and ‘family-to-work conflict’ (one item) at baseline: Scale from The General Nordic Questionnaire for Psychological and Social Factors at Work (QPS-Nordic)38; dichotomized into no conflict or more than some time during the week; Missing reliability | ‘Duration’ of medically certified long-term continuous sickness absence-period of at least 14 days from national social insurance registries. Participants were excluded if they were on disability pension at baseline. |
| Roelen et al. (2015) | 1557 Norwegian women (91%) and men with mean age 33.1 (SD:8.2); 1- and 2-year follow-ups | ‘Work-to-family’ (four items) and ‘family-to-work conflict’ (four items) at baseline and first follow-up: The Work–Family interface scale1; mean score; Cronbach alpha = 0.80 and 0.77. | ‘Duration’ of self-reported absence the last 12 months due to illness or injury at waves. High sickness absence was defined as > 30 days the past 12 months. Care-related sick leave for children or family members was excluded. |
| Vaananen et al. (2008) | 18366 Finnish women and men aged 20–64; 17 month (on average) follow-up | ‘Negative work-to-family spillover’ (three items) at baseline: Scale by Maardberg et al.39; Sum score categorized to three categories (high, moderate, low); Cronbach alphas > 0.80 | ‘Frequency’ of sickness absence from employers’ registries of more than 3 days during the follow-up computed as the number of absences per 100 and 1000 employee a year. |
| Vingård et al. (2005) | 6246 Swedish women up to age 61; 3-year follow-up | ‘General work–family conflict’ (two items) at baseline: One item each on work to family, and family to work conflict; Missing information on origin, use and reliability | ‘Frequency’ of employers-reported new spells of 28 or more days of consecutively sickness absence 3 years from baseline. |
| Voss et al. (2008) | 1583 Swedish women under age 50; 1-year follow-up | ‘General work–family conflict’ (two items) at baseline: Work negatively affecting home; and vice versa; Information on origin refers to the included study by Vingård et al.29 Dichotomized to the presence of work–family conflict when replying very often or always to at least one of the two items. | ‘Frequency’ of employer registered new sickness absence-spells during 2001 with (i) the number of subjects with four or more new sickness absence spells and (ii) long-term sickness absence with all spells longer than 28 days. |
Note: References to all scales are included as Supplementary Material.
Employer registries (n = 6)29,–33,35 and national social insurance registries (n = 1)34 were utilized to measure sickness absence. One study used self-reports on sickness absence.36 Operationalization varied from sickness absence frequency (i.e. number of episodes), duration (i.e. total number of days) and dimension (frequency of days) vs. categorization (with varying cut-offs). There was strong evidence for the association between gender and sickness absence with women reporting higher sickness absence than men regardless of operationalization and method (see table 2). See Supplementary Material for detailed information about findings in each study.
SIC and strength of evidence for all relationships examined
| Examined relationship | SIC-score | Strength of evidence |
|---|---|---|
| Women score higher: | ||
| Sickness absence (path c) | (8-0)/8 = 1 | Strong |
| Work-to-family conflict (path a1) | (2-0)/4 = 0.5 | Limited |
| Family-to-work conflict (path a2) | (2-0)/3 = 0.67 | Moderate |
| General work–family conflict (path a3) | 0 studies | Insufficient |
| Summarized: work–family conflict | (4-0)/7 = 0.57 | Moderate |
| Sickness absence is predicted by: | ||
| Work-to-family conflict (path b1) | (5-0)/8 = 0.63 | Strong |
| Family-to-work conflict (path b2) | (4-0)/7= 0.57 | Moderate |
| General work–family conflict (path b3) | (1-0)/4 = 0.25 | Inconsistent |
| Summarized: work–family conflict | (10-0)/19 = 0.53 | Moderate |
| Gender moderates: | ||
| Work-to-family conflict—>sickness absence (path d1) | (1-0)/4 = 0.25 | Inconsistent |
| Family-to-work conflict—>sickness absence (path d2) | (0-1)/3 = −0.33 | Limiteda |
| General work-to-family conflict—>sickness absence (path d3) | (0-0)/1 = 0 | Insufficient |
| Summarized: work–family conflict | (1-1)/8 = 0 | Insufficient |
| The gender gap in sickness absence is mediated by: | ||
| Work-to-family conflict (path c1’) | (1-0)/1 = 1 | Insufficient |
| Family-to-work conflict (path c2’) | (0-0)/1 = 0 | Insufficient |
| General work–family conflict (path c3’) | 0 studies | Insufficient |
| Summarized: work–family conflict | (1-0)/2 = 0.5 | Insufficient |
| Examined relationship | SIC-score | Strength of evidence |
|---|---|---|
| Women score higher: | ||
| Sickness absence (path c) | (8-0)/8 = 1 | Strong |
| Work-to-family conflict (path a1) | (2-0)/4 = 0.5 | Limited |
| Family-to-work conflict (path a2) | (2-0)/3 = 0.67 | Moderate |
| General work–family conflict (path a3) | 0 studies | Insufficient |
| Summarized: work–family conflict | (4-0)/7 = 0.57 | Moderate |
| Sickness absence is predicted by: | ||
| Work-to-family conflict (path b1) | (5-0)/8 = 0.63 | Strong |
| Family-to-work conflict (path b2) | (4-0)/7= 0.57 | Moderate |
| General work–family conflict (path b3) | (1-0)/4 = 0.25 | Inconsistent |
| Summarized: work–family conflict | (10-0)/19 = 0.53 | Moderate |
| Gender moderates: | ||
| Work-to-family conflict—>sickness absence (path d1) | (1-0)/4 = 0.25 | Inconsistent |
| Family-to-work conflict—>sickness absence (path d2) | (0-1)/3 = −0.33 | Limiteda |
| General work-to-family conflict—>sickness absence (path d3) | (0-0)/1 = 0 | Insufficient |
| Summarized: work–family conflict | (1-1)/8 = 0 | Insufficient |
| The gender gap in sickness absence is mediated by: | ||
| Work-to-family conflict (path c1’) | (1-0)/1 = 1 | Insufficient |
| Family-to-work conflict (path c2’) | (0-0)/1 = 0 | Insufficient |
| General work–family conflict (path c3’) | 0 studies | Insufficient |
| Summarized: work–family conflict | (1-0)/2 = 0.5 | Insufficient |
Note: Paths a–c’ corresponds with table 2.
Negative relationship with stronger associations for men.
SIC and strength of evidence for all relationships examined
| Examined relationship | SIC-score | Strength of evidence |
|---|---|---|
| Women score higher: | ||
| Sickness absence (path c) | (8-0)/8 = 1 | Strong |
| Work-to-family conflict (path a1) | (2-0)/4 = 0.5 | Limited |
| Family-to-work conflict (path a2) | (2-0)/3 = 0.67 | Moderate |
| General work–family conflict (path a3) | 0 studies | Insufficient |
| Summarized: work–family conflict | (4-0)/7 = 0.57 | Moderate |
| Sickness absence is predicted by: | ||
| Work-to-family conflict (path b1) | (5-0)/8 = 0.63 | Strong |
| Family-to-work conflict (path b2) | (4-0)/7= 0.57 | Moderate |
| General work–family conflict (path b3) | (1-0)/4 = 0.25 | Inconsistent |
| Summarized: work–family conflict | (10-0)/19 = 0.53 | Moderate |
| Gender moderates: | ||
| Work-to-family conflict—>sickness absence (path d1) | (1-0)/4 = 0.25 | Inconsistent |
| Family-to-work conflict—>sickness absence (path d2) | (0-1)/3 = −0.33 | Limiteda |
| General work-to-family conflict—>sickness absence (path d3) | (0-0)/1 = 0 | Insufficient |
| Summarized: work–family conflict | (1-1)/8 = 0 | Insufficient |
| The gender gap in sickness absence is mediated by: | ||
| Work-to-family conflict (path c1’) | (1-0)/1 = 1 | Insufficient |
| Family-to-work conflict (path c2’) | (0-0)/1 = 0 | Insufficient |
| General work–family conflict (path c3’) | 0 studies | Insufficient |
| Summarized: work–family conflict | (1-0)/2 = 0.5 | Insufficient |
| Examined relationship | SIC-score | Strength of evidence |
|---|---|---|
| Women score higher: | ||
| Sickness absence (path c) | (8-0)/8 = 1 | Strong |
| Work-to-family conflict (path a1) | (2-0)/4 = 0.5 | Limited |
| Family-to-work conflict (path a2) | (2-0)/3 = 0.67 | Moderate |
| General work–family conflict (path a3) | 0 studies | Insufficient |
| Summarized: work–family conflict | (4-0)/7 = 0.57 | Moderate |
| Sickness absence is predicted by: | ||
| Work-to-family conflict (path b1) | (5-0)/8 = 0.63 | Strong |
| Family-to-work conflict (path b2) | (4-0)/7= 0.57 | Moderate |
| General work–family conflict (path b3) | (1-0)/4 = 0.25 | Inconsistent |
| Summarized: work–family conflict | (10-0)/19 = 0.53 | Moderate |
| Gender moderates: | ||
| Work-to-family conflict—>sickness absence (path d1) | (1-0)/4 = 0.25 | Inconsistent |
| Family-to-work conflict—>sickness absence (path d2) | (0-1)/3 = −0.33 | Limiteda |
| General work-to-family conflict—>sickness absence (path d3) | (0-0)/1 = 0 | Insufficient |
| Summarized: work–family conflict | (1-1)/8 = 0 | Insufficient |
| The gender gap in sickness absence is mediated by: | ||
| Work-to-family conflict (path c1’) | (1-0)/1 = 1 | Insufficient |
| Family-to-work conflict (path c2’) | (0-0)/1 = 0 | Insufficient |
| General work–family conflict (path c3’) | 0 studies | Insufficient |
| Summarized: work–family conflict | (1-0)/2 = 0.5 | Insufficient |
Note: Paths a–c’ corresponds with table 2.
Negative relationship with stronger associations for men.
Work–family conflict were measured by self-reports in all studies. Four of the included studies examined work-to-family and family-to-work conflict separately,31–34,36 one study examined family-to-work conflict only,35 and two studies examined general work–family conflict.29,30 There was moderate evidence for the association between gender and all work–family conflict measures with women reporting higher sickness absence than men (see table 2). Women reported significantly higher work-to-family conflict32,34 and family-to-work conflict than men.31,32 No effect sizes were reported.
With regard to study quality, all studies inhabited methodological strengths in using employer- or national registries to measure sickness absence, appropriate follow-up periods, large samples and lowered risk of common method bias by using both self-reports and registry data (see Supplementary Table S1). The majority of the studies (75%) adjusted for potential confounders. Still, about half of the studies (43%) had an acceptable response rate at baseline level and only half of the studies examined work–family conflict in a valid and/or reliable manner. Moreover, all of the studies examined work–family conflict only at baseline and not at more time points, which is useful for the examination of temporal causality.
H1: We found moderate evidence for a prospective association between work–family conflict measures and subsequent sickness absence (see table 2).
The strength of evidence indicates a strong level of evidence for work-to-family conflict and a moderate level of evidence for family-to-work conflict. The strength of the associations ranged from small (β = 0.06)31 to (OR = 1.48)32 for work-to-family and family-to-work conflict. There was an inconsistent evidence for the link between general work–family conflict (i.e. no direction or sum of both directions) and sickness absence, with reports of both insignificant findings29,33 and a medium-sized association (RR = 1.55).30 See supplementary data for more detail about each study.
H2: There was insufficient evidence for the prospective association between work–family conflict-measures and sickness absence to be moderated by gender (see table 2).
Four studies examined gender moderation with either significance testing the differences or included confidence intervals for separate analyses for men and women.32–35 Stronger associations between work–family conflict and sickness absence were reported for men in one study32 and women in another study,33 while the other two studies reporting no differences.34,35 There were limited evidence for a stronger relationship between family-to-work conflict and sickness absence for men. See Supplementary Material for more detail about each study. Three studies examined more complex sub-groups.28,34,35 When sub-groups were analysed separately, findings suggested strongest associations for women who had the main housework responsibility,34 were single mothers30 and for men who have high socioeconomic status (SES).34 However, interaction analyses to support group differences were not performed, and risk of Type I-errors in multiple sub-group comparisons cannot be excluded.
H3: There was insufficient evidence for the association between gender and sickness absence to be mediated by work–family conflict (see table 2).
The findings from the included studies indicate moderate level of evidence for gender to predict work–family conflict and for work–family conflict to predict sickness absence, which are two of the criterions for mediation. Still, only one of the studies examined family stressors as a mechanism of the gender gap in sickness absence.31 In this study, family-to-work conflict, but not work-to-family conflict, was a partial mediator between gender and sickness absence duration and frequency in mediation analyses before and after conducting adjustments for other potential mediators (e.g. job characteristics and strain) and confounders.
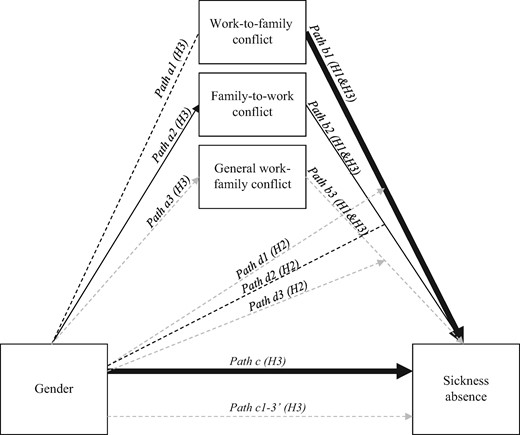
The level of evidence based on SIC for the longitudinal associations between gender, work–family conflict and sickness absence. Bold line, strong evidence; normal line, moderate evidence; dotted line, limited evidence; dotted grey line, insufficient or inconsistent evidence. H1, Hypothesis 1; H2, Hypothesis 2; H3, Hypothesis 3
Discussion
The aim of this study was to shed light on the double burden hypothesis of sickness absence by systematically reviewing studies of perceived work–family conflict, rather than studies counting number of children or role memberships. We found moderate evidence for a positive relationship between work–family conflict and subsequent sickness absence, which extends upon former cross-sectional findings,18 and thus lends support for the double burden and role strain theory for sickness absence. The quality assessment showed that each study scored low on at least one quality assessment point; low response rate and/or low validity/reliability of the work–family conflict measure. One can thus speculate if the strength of the evidence and/or associations between work–family conflict and sickness absence would have been stronger if the studies had higher quality in these aspects. Moreover, despite the prospective longitudinal design in all included studies improving upon former cross-sectional systematic reviews, none of the included studies measured work–family conflict at follow-up. Thus, we cannot rule out bidirectionality/reverse causation, and we strongly encourage future studies to include measurements of work–family conflict at several time points.
In line with former studies,3–6 women consistently had higher sickness absence rates than men, regardless of operationalizations, samples and study country. There was however inconsistent evidence whether the effect of gender moderates the relationship between work–family conflict measures and sickness absence. Associations were sometimes found to be stronger for men,32 sometimes for women,33 and sometimes non-significant.34,35 There were some indications for stronger associations between work–family conflict and sickness absence for subgroups, such as women with a more demanding domestic34 or occupational situation (i.e. ‘blue collar professions’).35 This is in line with a recent finding indicating that work demands were more strongly associated with work–family conflict for those with caregiving status (i.e. child and parent caregiving) regardless of gender.40 Only some of the included studies30,33,34 adjusted for, or took into consideration, family-related factors such as domestic responsibilities, partner or parent status, number of children or age of children. However, we warrant strict caution when interpreting these findings due to their exploratory nature and high risk of type 1-error. The findings still offer some directions to what factors future studies could focus on when examining sickness absence.
There were an insufficient number of studies to examine if work–family conflict mediated the relationship between gender and sickness absence, with only one of the included studies doing so. In that study, family–work conflict partially explained the association between gender and sickness absence,31 but only a small portion of variance (i.e. 5–9%) was accounted for by work–family and family–work conflict together with five other variables (e.g. job characteristics and strain, and social support). In similar lines, another study reported that a minimal proportion of the association between gender and sickness absence was accounted for by family-related factors (i.e. marital status, number of children, work–family conflict, negative life events, partner conflict, social networks and support).7 Considering the well-documented findings that women have higher sickness absence than men, it is surprising that only one of the included studies examined mechanisms of the gender gap.31 There was some evidence (limited to moderate) that women report higher work–family conflict than men. This link (gender and work–family conflict) together with the association between work–family conflict and sick leave suggests that there might be mediation present, which should be examined in further studies.
Despite the fact that the studies originated from countries with high degrees of gender equality (e.g. Netherlands, Belgium and Nordic countries), women mostly reported higher work–family conflict. Thus, high gender equality in labour force participation might lead to lower gender equality in other areas (i.e. caregiving and domestic responsibility). Other countries might have less work family conflict and sick leave due to lower labour force participation in females, but maybe higher degree of economic dependency and higher poverty.
Most of the included studies combined self-reported work–family conflict with registry data of sickness absence, lowering the risk of common method bias. There are still limitations to be considered. First, the response rates were low, approaching <50% in about half of the studies.31–33 There is therefore a chance that those with the highest levels of work–family conflict and sick leave were absent (i.e. ‘healthy worker effect’). However, recent findings from a two-wave study indicate few differences in baseline somatic and mental health problems in responders vs. non-responders.41 Despite low education level predicting dropout, baseline associations between health and work factors remained the same in responders and non-responders. Even though these findings do not support the ‘healthy worker effect’, using national registries or individual contact instead of employer registries at follow-up would reduce this threat in future studies.
Second, all studies were conducted in quite homogenous high-income Northern European countries with relatively high social security and favourable welfare policies, proposing caution in generalizations to other cultures. Additionally, comparisons between Northern European countries and the included studies were difficult, as national policies often is the basis of the operationalization of sickness absence. Future studies should thus include the use of several different operationalizations of sickness absence to assess the robustness of the results. Future studies could improve upon the methodological standards for the measurement of work–family conflict.29,30,34 However, former meta-analyses have noted that there is an ambiguity in the measurement and nature, which might lie behind inconsistencies in findings.17 Some former noted problems have been single-item measurements, unknown validity and differences in the focus in different operationalization. Despite most studies not using single-item measurements anymore, there is a need for improvement on validity/reliability in the work–family conflict measures today.
All included studies relied on self-reported work–family conflict, which warrants some caution. For instance, both mental and somatic health problems could affect both actual and perceived work–family conflict as well as sickness absence. On the other side, adjusting for such health problems, which also could be a potential mechanism for how work–family conflict leads to sickness absence, could lead to underestimation of actual effects.
The current review utilized a transparent systematic approach of searching, screening and quality assessing the studies according to pre-defined criteria with no time or language restrictions. Still, there are some limitations to be discussed. The few included studies warrants caution, but due high sample sizes within the studies, power is not an issue. Still, quantitatively summing up the findings using SIC-scores27,28 warrants some caution. One study representing 45% of the total sample size is not being taken into consideration in scores.35 This study thoroughly reviewed studies examining work–family conflict and sickness absence, and did not focus on other predictors of sickness absence. It must thus be emphasized that no single factor alone can explain sickness absence or the gender gap thereof, and that multiple factors from different levels (e.g. individual, societal) and contexts (e.g. work, family) should be examined to fully understand the aetiology of sickness absence.
Conclusions
Despite the increasing interest in family stressors and work outcomes, this is the first systematic review of longitudinal associations between work–family conflict and subsequent sickness absence. The findings lend moderate support to a generalized model where double burden, measured by either work-to-family or family-to-work conflict, is associated with subsequent sickness absence in both women and men. This also suggests focusing on the family context when assessing individuals with sickness absence at the work place and health care services. Women reported more work–family conflict than men indicating that work–family conflict contribute somewhat to the gender gap in sick leave. This was supported in one study and cannot yet be supported nor dismissed. Higher quality designs such as higher response rates, and examining methodologically valid work–family conflict measurements at more than one time point are needed in future studies to examine this further.
Supplementary data
Supplementary data are available at EURPUB online.
Acknowledgement
We wish to thank librarian Wenche Jacobsen at the Norwegian Institute of Public Health for teaching us systematic search strategies and for being such a nice person.
Funding
Research Council of Norway’s Programme for Sickness Absence, Work and Health (SYKEFRAVÆR) [Grant project number 218373].
Conflicts of interests: None declared.
Key points
Eight longitudinal studies of work–family conflict and sickness absence were included screening more than 2200 studies
There were moderate level of evidence for work–family conflict to prospectively be associated with sickness absence—suggesting a potential double-burden of combining work and family.
The findings suggest to also focusing on the family context when assessing individuals with sickness absence at the work place and health care services.
Women reported higher work–family conflict than men.
There were too few studies and insufficient evidence to support the double-burden hypothesis for the gender gap in sickness absence.
References

{kind=link}
{kind=link}
Comments