

Can Kids Get Seriously Ill With Covid?

Stuff Does It Again – A Horror Headline Hanging by a Thread
Stuff’s article implies that more children are getting seriously ill with Covid-19 and should be vaccinated, citing an international study. However, there are a number of gaping holes not only in Stuff’s reporting but also in the study cited.
This is what the study actually says.
“Although the overall proportion of SARS-CoV-2–negative youths who experienced severe outcomes did not differ from that among test-positive youths, among hospitalized children, those who were SARS-CoV-2 positive were more likely to experience severe outcomes.”
The Study
January 11, 2022
Outcomes of SARS-CoV-2–Positive Youths Tested in Emergency Departments The Global PERN–COVID-19 Study
Anna L. Funk, PhD, MSc1; Todd A. Florin, MD, MSCE2,3; Nathan Kuppermann, MD, MPH4; et al
Conflicts of interest.
- Dr Florin reported receiving grants from the National Institute of Allergy and Infectious Diseases (NIAID, of which Tony Fauci is the director) and the National Heart, Lung, and Blood Institute outside the submitted work.
- Dr Ambroggio reported receiving grants from Pfizer outside the submitted work.
- Dr Malley reported receiving personal fees from Merck as a consultant, grants from Pfizer, grants from Astellas, and reported being a board member and consultant for Affinivax Scientific Founder outside the submitted work.
- Dr Morris reported royalties from intellectual property from UCSF Benioff Children’s Hospital Oakland; grants from NIH/NHLBI, grants from FDA, and grants from NIH/NCCIM outside the submitted work; in addition, Dr Morris had a patent for therapeutics related to Arginine bioavailability in COVID-19 and MISC pending.
- Dr Becker reported receiving Primary Children’s Hospital Fee per enrolled study participant from University of Utah during the conduct of the study.
No other disclosures were reported. Researchers will often check whether the authors of published studies have conflicts of interest that could affect the way they interpret their data. As you can see here, there is significant conflict of interest. It is worth pointing out that the doctors and scientists of NZDSOS gain nothing by standing up and speaking out. Many of us have lost jobs and possibly careers. Yet, we continue to speak out as we cannot stand idly by while harms are being committed in our names as doctors.
Children in the study.
There are significant concerns about the way in which the data collected for the purposes of this study have been presented in JAMA (Journal of the American Medical Association) Network Open.
This study was designed as a multi-centred prospective cohort study and data was collected at 41 Emergency departments across 8 countries. Argentina, Canada, Costa Rica, Italy, Paraguay, Singapore, Spain, and the United States. There is no mention of New Zealand’s part in the study, as stated by Stuff.
All patients recruited to the study were under 18 years of age and presented with symptoms of febrile respiratory illness (fever, cough, rhinorrhoea, congestion, wheezing, difficulty breathing, sputum production, sore throat, or apnoea). The study placed emphasis on the development of severe clinical outcomes as the selected endpoints. These are defined to include: cardiac or cardiovascular (cardiac arrest, cardiac ischemia, congestive heart failure, endocarditis, myocarditis, pericarditis, stroke), infectious (disseminated intravascular coagulation, mastoiditis, sepsis with bacteraemia, septic shock, toxic shock syndrome), neurologic (encephalitis, meningitis), respiratory (acute respiratory distress syndrome, empyema, necrotizing or cryptogenic organizing pneumonia, pleural effusion or pneumothorax or pneumomediastinum requiring drainage, respiratory failure), and death. In the description of the studies objectives the authors report making a comparison in the frequency of severe clinical outcomes in subjects who returned a positive SARS-CoV-2 PCR test compared to those who returned a negative PCR test.
There were 10 382 study participants in total, 3222 (31%) tested positive for SARS-CoV-2 during the study period. The larger group of 7160 (69%) participants failed to return a positive SARS-CoV-2 PCR test during the study period. A fair representation of the data collected over the course of the study would have shown clinical outcomes for both arms of the study. It is striking that every published chart, table figure and diagram the published in the body of the study pertain only to the smaller study sub-group (those that returned a positive PCR test). The flow diagram (Figure 1 in the publication) copied below provides an illustration of this point. The data pertaining to the entire PCR negative arm of the study is not represented plainly in the publication and can only be found in the online supplemental material.
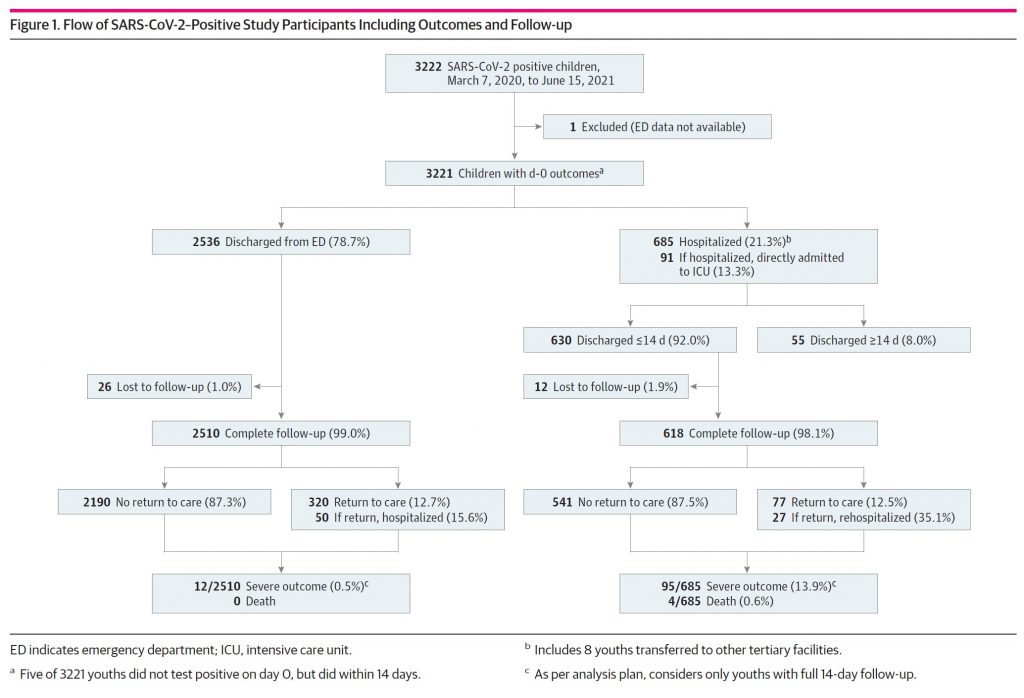
The Interpretation
Unfortunately, this study exemplifies significant reporting bias as it selectively and asymmetrically emphasizes one arm of the study over the other. The presentation of data is largely confined to those participants that returned a positive PCR Test for SAR-CoV-2 with very little attention paid to the other arm of the study in which all subjects presented with the same constellation of severe respiratory symptoms but returned a negative PCR test for SAR-CoV-2. The following statement reveals what should be the most relevant finding in this comparative study.
“Although the overall proportion of SARS-CoV-2–negative youths who experienced severe outcomes did not differ from that among test-positive youths, among hospitalized children, those who were SARS-CoV-2 positive were more likely to experience severe outcomes.” (Our emphasis)
In hospitalised patients with the positive PCR test the risk of a severe outcome was elevated by 3.9% (95% CI, 1.1%-6.9%). As no information was provided about the specifics of the treatment provided to study participants on the basis of their PCR status, it is not possible to ascertain whether the treatment provided to PCR positive patients differed from that provided to the PCR negative patients in a meaningful way. Some of the treatments used in the management of Covid-19 have been shown to be be associated with unfavourable outcomes.
Main Stream Media Reporting
The above study has recently been cited by main-stream media sources to bolster public support for the vaccination roll out in children (5–12-year-old age). There seems to have been a recent emphasis placed upon the occurrence of severe disease in children due to Covid-19 (the clinical syndrome associated with infection with the SARS-CoV-2 infection). Stuff’s headlines scream: “Covid-19: Study shows kids can get seriously ill, should be vaccinated – researcher”. The timing of this newly emerging narrative appears contrived due to it’s tight coupling with the vaccine roll-out in children. Nowhere in the study is vaccination mentioned, contrary to Stuff’s headline. Not one month ago, Stuff drew attention to a child in New Zealand under 10, with this misleading headline: “Coivd-19: Child under 10 becomes youngest case to die”. This child tested positive after death. Surely in the middle of a pandemic, any child with respiratory symptoms would be immediately tested for Covid-19? The case is still under investigation and until we know more, this unfortunate death cannot be said to be due to Covid-19.
Another Trial: Trivial Increase in GP Visits
An interesting paper from Norway looked at over 700 000 children aged between 1 and 19 years old before the Covid-19 vaccination was commenced. They looked at whether Primary Care (GP) or specialist visits were increased in those who had a test for Covid-19. The authors state that:
In 706 885 children and adolescents who were or were not tested for SARS-CoV-2 in Norway, we found that those aged 1-19 years had symptoms severe enough to increase their use of primary, but not specialist, care after a positive test result…Our findings could thus imply that because no specialist care was needed the severity of post-covid symptoms is limited in children.
Covid-19 among children and adolescents has a limited impact on healthcare services. Preschool aged children might take longer to recover (~3-6 months) than primary or secondary school students (~1-3 months), usually because of respiratory conditions. The limited impact of covid-19 on the health of young people is important information in the consideration of whether children and adolescents should be vaccinated to protect themselves and others.
(our italics)
This study was undertaken between 1 August 2020 and 1 February 2021, well before Omicron was present. The figures for Omicron are likely to be much less. Less doctor’s visit indicates a less severe disease. In fact, there was only a trivial increase in doctor’s visits. This needs to be weighed up against the potential harms of the vaccine.
The Omicron variant is strongly pushed in the media at present due to it high transmissibility, meaning it is easily passed from one person to the next. However, it behooves us all to take a deep breath and understand that Omicron is a mild disease with a trivial case fatality rate. Furthermore, if it is contracted, it may provide immunity against other variants. This cannot be said for the C-19 injections which neither prevent infection nor spread it. Even worse, the Covid-19 injections may weaken your immune system and may cause severe side-effects.
We ask yet again, why the main-stream media is not looking at all the data. It is time to turn them off
What Kids Can Do
Keep healthy by visiting family and getting lots of hugs and laughs, as this helps to boost the immune system. Eat well, exercise and get outside for some sun, without burning. Not only will you have a better chance of not even noticing Omicron or any other variant, but you will be stronger and happier, for yourself, your family and your community.



2 Comments
Comments are closed.