Recycling the Purpose of Old Drugs to Treat Ovarian Cancer


1
Differentiation and Cancer Group, Institute for Research and Innovation in Health (i3S) of the University of Porto/Institute of Molecular Pathology and Immunology of the University of Porto (Ipatimup), 4200-135 Porto, Portugal
2
Porto Comprehensive Cancer Center (PCCC), 4200-162 Porto, Portugal
3
Department of Medical Oncology, Portuguese Oncology Institute of Porto (IPOP), 4200-162 Porto, Portugal
4
Department of Pathology, Portuguese Oncology Institute of Porto (IPOP), 4200-162 Porto, Portugal
5
Cancer Biology & Epigenetics Group, Research Center—Portuguese Oncology Institute of Porto (CI-IPOP), 4200-162 Porto, Portugal
6
Faculty of Medicine, University of Porto, 4200-319 Porto, Portugal
7
Department of Sciences, University Institute of Health Sciences (IUCS), CESPU, CRL, 4585-116 Gandra, Portugal
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2020, 21(20), 7768; https://doi.org/10.3390/ijms21207768
Submission received: 14 September 2020 / Revised: 13 October 2020 / Accepted: 17 October 2020 / Published: 20 October 2020
(This article belongs to the Special Issue Gynecologic Oncology: From Molecular Mechanisms to Targeted Therapies 2.0)
Abstract
:
The main challenge in ovarian cancer treatment is the management of recurrences. Facing this scenario, therapy selection is based on multiple factors to define the best treatment sequence. Target therapies, such as bevacizumab and polymerase (PARP) inhibitors, improved patient survival. However, despite their achievements, ovarian cancer survival remains poor; these therapeutic options are highly costly and can be associated with potential side effects. Recently, it has been shown that the combination of repurposed, conventional, chemotherapeutic drugs could be an alternative, presenting good patient outcomes with few side effects and low costs for healthcare institutions. The main aim of this review is to strengthen the importance of repurposed drugs as therapeutic alternatives, and to propose an in vitro model to assess the therapeutic value. Herein, we compiled the current knowledge on the most promising non-oncological drugs for ovarian cancer treatment, focusing on statins, metformin, bisphosphonates, ivermectin, itraconazole, and ritonavir. We discuss the primary drug use, anticancer mechanisms, and applicability in ovarian cancer. Finally, we propose the use of these therapies to perform drug efficacy tests in ovarian cancer ex vivo cultures. This personalized testing approach could be crucial to validate the existing evidences supporting the use of repurposed drugs for ovarian cancer treatment.
{kind=link}
{kind=link}
{kind=link}
1. Introduction
Ovarian cancer (OC) is the leading cause of gynaecological cancer-related mortality worldwide [1,2]. In Europe, 67,800 women are diagnosed with OC and 44,600 die from this malignancy annually [3]. The most prevalent subtype, high-grade serous carcinoma (HGSC), is particularly lethal, since it develops rapidly and often presents with advanced stage disease [4,5,6]. Treatment options are limited, and typically involve cytoreductive surgery and platinum-based chemotherapy [4,5,6,7]. While many patients initially respond well, approximately 75% of women develop incurable recurrences, contributing to poor survival rates that have not changed substantially for the past years [8]. The main challenge in OC is to unveil a therapeutic strategy to overcome chemoresistance. Many targeted therapies have been approved to treat OC, e.g., poly (ADP-ribose) polymerase (PARP), and vascular endothelial growth factor (VEGF) inhibitors; however, the median progression-free survival (PFS) remains poor [9,10,11]. Even in platinum sensitive relapse and considering only the best responders, the addition of bevacizumab or PARP inhibitors (iPARPs) correlates with a PFS no longer than 21 months [12,13,14,15,16]. Here, we propose an alternative approach based on the use of non-oncological drugs for OC treatment. This concept, called drug repurposing, is based on the knowledge of pharmacokinetics, pharmacodynamics, target identification, bioavailability, toxicity profiles, recommended dosage schemes, and consistent recognition of adverse effects, meaning that oncological indication development can begin at phase II of the clinical trials, making the research process less time-consuming and less expensive [17,18,19,20]. The incorporation of non-oncological drugs for cancer treatment is usually combined with chemotherapeutic agents, target therapies, or other repurposed drugs [21].
In the OC setting, many non-oncological drugs have promising in vitro results and some of them already being tested in clinical trials. These therapeutic compounds include antifungal (itraconazole), antilipidemic (statins), antidiabetic (metformin), antiviral (ritonavir), antiparasitary (ivermectin) drugs, and osteoporosis treatment (bisphosphonates). In this review, we gather information about the most promising drug repurposing strategies for OC treatment and propose a strategy to test these therapeutic options in patient-derived samples.
2. Drug Repurposing for Ovarian Cancer Therapy
2.1. Statins
Statins are inhibitors of 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR), located upstream in the mevalonate pathway, which is responsible for cholesterol biosynthesis [22,23,24]. The main clinical use of statins is to reduce plasma cholesterol levels, being a key treatment in the prevention of cardiovascular diseases [25,26,27,28,29]. Statins can also reduce inflammation, influence vascular expansion and remodelling, and inhibit coagulation and fibrinolysis [30,31,32].
The inhibition of HMGCR leads to a cascade of inhibition in downstream proteins (i.e., geranyl pyrophosphate, farnesyl pyrophosphate, and geranylgeranyl pyrophosphate), that play important roles in several signalling pathways, such as membrane trafficking, cell motility, proliferation, differentiation, and cytoskeletal organization [33]. HMGCR is considered a metabolic oncogene as it promotes tumour growth and co-operates with rat sarcoma virus (RAS) to transform cells in colony forming assays [34]. Retrospective studies suggest that statins exhibit an anti-tumoral effect and are associated with a decreased risk of recurrence in several neoplasms, including breast and ovarian cancers [26,35,36,37,38,39,40,41,42,43,44].
In OC setting, it has been demonstrated that statins reduce cell proliferation and migration in vitro leading to a delay in tumour formation and suppress the metastatic capacity in vivo [45,46,47]. Several others experimental studies, using OC cell lines and animal models, demonstrate that statins block the cholesterol biosynthesis leading to apoptosis and tumour cell differentiation, proliferation, invasion, migration, angiogenesis and metastasis, through the activation of multiple signalling pathways [35,36,46,48,49,50,51,52]. Martirosyan et al., demonstrated that lovastatin triggers apoptosis of OC cells as a single agent by blocking HMGCR activity (mevalonate-dependent mechanism) and sensitizing chemoresistant cells to doxorubicin by blocking drug efflux pumps (mevalonate-independent mechanism) (Figure 1) [35]. A recent study performed by Dr Richardson’s group, found that pitavastatin, a lipophilic statin with a long half-life, was able to inhibit the growth of two-dimensional (2D) and three-dimensional (3D) OC cell cultures with a resistant profile to carboplatin, suggesting that pitavastatin has a great potential to treat chemoresistant tumours [53]. Additionally, this study showed that high expression of wild type and gain-of-function tumour protein 53 (TP53) variants led to an increased HMGCR expression [53]. This observation is particularly important in HGSC, where dysregulation of TP53 is an almost ubiquitous event [54,55,56], suggesting that a significant proportion of OC patients could benefit from pitavastatin treatment [53,57].
Regarding OC survival studies, the overall survival (OS) rate for post diagnostic patients is significantly higher in statins users (hazard ratio (HR)) = 0.63; 95% confidence interval (CI) = 0.54–0.74 [58]; HR = 0.87; 95% CI = 0.80–0.95 [59]) compared to non-users. Other studies show that statin users present all-cause mortality and cancer-related mortality rates significantly lower (HR = 0.72; 95% CI = 0.56–0.93 [60]; HR = 0.85; 95% CI = 0.82–0.87 [61]) compared to non-users. A recent study demonstrated that patients who started a statin treatment after being diagnosed with OC had a significant reduced risk of all mortality (adjusted HR = 0.81; 95% CI = 0.72–0.90) compared to non-users, being associated with improved survival [62]. Several other studies show evidences for a significant reduction in OC risk among statin users compared to non-users [26,51,62,63]. In fact, for 13 types of cancers, it was observed a decrease in cancer-related death risk in statin users [61]. The anti-tumoral effects of statins has also been described in variety of other cancer origins, for example, endometrial cancer (HR = 0.83; 95% CI = 0.69–1.01) [58], breast cancer (HR = 0.81; 95% CI = 0.68–0.96) [64], colorectal cancer (fully adjusted HR = 0.71; 95% CI = 0.61–0.84) [65] and prostate cancer (HR = 0.76; 95% CI = 0.66–0.88) [66]. These studies show the effect of statins to prevent the onset of cancer.
Several experimental and observational studies suggest that statins could exhibit anticancer properties or being used as adjuvants to the current OC therapeutic options [67]. In concordance, ongoing clinical trials are testing the effects of different statins in the treatment of OC patients (Table S1). Statins efficacy has been studied for as cancer treatment as monotherapy or combinatorial therapy, being the last option the most effective [47,68,69,70,71,72].
Statins are one of the most commonly used drugs worldwide to treat cardiovascular diseases. The results on its putative use in OC prevention/recurrence and in a chemoresistant setting are promising but there is much to improve regarding the type of statins, its half-life and dosage.
2.2. Metformin
Metformin is used in the treatment of type 2 diabetes since induces anti-hyperglycaemia, mainly through the decrease of insulin resistance and blocking glucose-6-phosphatase that reduces hepatic gluconeogenesis and inhibit gastro-intestinal glucose reabsorption [73,74,75,76]. Metformin inhibit the respiratory-chain complex 1, induce a drop in cellular energy charge, activate glucose uptake through promoting glucose transporter type 4 translocation to the plasma membrane that mediates the activation of liver kinase B1 and adenosine monophosphate-activated protein kinase (AMPK) [75,76,77,78]. Consequently, cellular adenosine triphosphate (ATP) concentrations fall, and the increase in both adenosine diphosphate (ADP)/ATP and adenosine monophosphate (AMP)/ATP ratios triggers AMPK that coordinates a wide range of compensatory, protective, and energy sparing responses, leading to a reduction in hepatic glucose output [75,76,77,78]. Metformin inhibits cell proliferation and insulin signals, blocks protein and fatty acid synthesis, and exhibits anti-inflammatory properties [79,80]. Besides that, it has also been reported that metformin has anti-tumoral properties, since the inhibition of the glucose production will cause alterations in metabolic and endocrine circuits that change some cellular and molecular processes that will influence cancer biology causing oxidation stress and deoxyribonucleic acid (DNA) damage [17,79,81].
Many mechanisms of metformin’s anti-cancer activity have been proposed. Some studies suggest that metformin modulate the immunological and/or anti-inflammatory responses in cancer treatment [82,83]. Other studies demonstrate that metformin inhibit mammalian target of rapamycin (mTOR) through activation of AMPK resulting in reduced cancer cells proliferation [84,85]. Metabolic actions have been proposed related to gluconeogenesis, mitochondrial function, and cellular metabolism [86,87]. Metformin reduces cellular respiration by inhibiting respiratory-chain complex 1 limiting the cancer cell’s metabolic plasticity [73,88,89]. However, cancer cells try to compensate the suppression of oxidative phosphorylation by enhancing glycolysis that is p53-dependent [89]. HGSC normally present absence of functional p53; therefore, cancer cells are incapable to compensate for metformin-induced suppression of oxidative metabolism [90]. In OC, metformin is reported to reverse chemoresistance, avoid epithelial mesenchymal transition (EMT), reduce cancer cell migration, and metastasis [87,91,92,93,94]. In fact, in this tumoral context, several studies demonstrate that metformin blocks cell growth, induces apoptosis, inhibits angiogenesis and metastatic spread, potentiates effectivity of chemotherapeutic agents, and reverses chemoresistance (Figure 1) [77,86,92,95,96,97,98,99,100,101,102,103]. Besides that, metformin, either alone or in combination with cisplatin, inhibit cell viability and angiogenesis, and induces apoptosis in OC cell lines [104]. Another in vitro and in vivo study demonstrated that combining iPARPs and metformin enhances the anti-tumoral effects regardless of breast cancer (BRCA) status [105].
Epidemiological studies reveal that cancer-related mortality rate is significantly lower in metformin patient users and that survival rates is improved in many types of cancer patients, i.e., colorectal, pancreatic, breast, liver and endometrial cancers [106,107]. A recent study demonstrated that metformin significantly prolonged the OS (HR = 0.61; 95% CI = 0.48–0.77) and reduced recurrence risk (HR = 0.50; 95% CI = 0.28–0.92) in endometrial cancer [108]. Regarding endometrial cancer, results showed that metformin amplify the effects of paclitaxel by blocking mTOR-signalling pathway [109]. Other epidemiological studies and meta-analysis demonstrate that metformin reduce OC risk (odd ratio (OD) = 0.61; 95%CI = 0.30–1.25 [110]; OD = 0.57; 95%CI = 0.16–1.99 [111]) and OC-specific mortality [110,111,112,113,114,115,116]. In addition, the 5-years PFS was significantly better for OC patients with type 2 diabetes who were taking metformin (63%) compared to users of other hypoglycaemic drugs (37%) and non-users (23%) (p = 0.03) [112]. Corroborating these results, another study demonstrated that 5-years survival rate was significantly better in the group of metformin users (67%) compared to non-users (47%) and that metformin remained an independent predictor of survival (HR = 2.2; 95% CI = 1.2–3.8) [115]. A recent meta-analysis demonstrated that the metformin use in post-diagnostic OC patients is associated with improved OS (summarized HR = 0.42; 95%CI = 0.31–0.56) and PFS (summarized HR = 0.69; 95% CI = 0.45–1.07) regardless of diabetes status [117]. Several others retrospective studies reached similar conclusions, indicating that cancer patients with diabetes treated with metformin presented a substantially lower cancer burden than patients with diabetes treated with other antilipidemic drugs [118,119,120,121,122]. In vivo studies demonstrate that metformin can target ovarian cancer stem cells (CSCs) and, therefore, enhance chemotherapy response [103,123] proposing a mechanism of action based on CSC targeting [92,103,124,125,126,127,128].
A recent phase II clinical trial show a median PFS of 18.0 months (95% CI = 14.0–21.6) with a relapse-free survival at 18 months of 59.3% (95% CI = 38.6–70.5) and a median OS of 57.9 months (95% CI = 28.0-not estimable) for metformin users in non-diabetic OC patients [129]. The same authors demonstrate that metformin is a CSC targeting agent, since metformin-treated ex vivo tumours exhibit an average 2.4-fold decrease in ALDH+/CD133+ cells and an increased sensitivity to cisplatin compared to non-metformin-treated cells [129].
A phase I clinical trial is currently testing the effect of metformin in combination with carboplatin-paclitaxel chemotherapy in advanced OC and evaluating its safety and pharmacokinetics [130]. Additionally, a randomized phase-II trial is being conducted to evaluate metformin as a maintenance therapy in combination with standard chemotherapy in stage III–IV ovarian, fallopian tube or primary peritoneal cancer patients (NCT02122185).
Ongoing clinical trial are currently testing this therapeutic option the OC setting being determinant to unveil the role of metformin in the OC treatment (Table S1). Many experimental and epidemiological results emphasize the utility of metformin in oncology management, suggesting its potential role in the treatment of advanced OC, especially when combined with platinum compounds.
2.3. Bisphosphonates
Bisphosphonates (e.g., alendronate and zoledronic acid) are widely used to treat osteoporosis through inhibition of bone resorption by decreasing osteoclast activity [131,132]. Bisphosphonates blocks farnesyl pyrophosphate synthase located downstream than HMGCR in the mevalonate pathway [133]. Farnesyl pyrophosphate is an enzyme involved in the synthesis of compounds that are necessary for maintaining osteoclast function, such as farnesyl pyrophosphate and geranylgeranyl pyrophosphate [134]. Bisphosphonates have an effect in prevention of specific clinical complications of bone metastasis (hypercalcemia, bone fractures, and pain) and have an additional anti-metastatic and anti-tumoral property when combined with chemotherapeutic agents inhibiting tumour proliferation and dissemination [134,135,136,137,138]. In vitro experiments, using breast and prostate cancer cell lines, demonstrate that bisphosphonates promote apoptosis and block cell proliferation [139,140]. In addition, studies using OC cell lines and animal models have shown that bisphosphonates have an anti-proliferative and pro-apoptotic activity through the inhibition of cell proliferation and angiogenesis, induction of apoptosis, and activation of immune cells [141,142,143,144,145,146]. A recent study demonstrated that bisphosphonates inhibit OC cell lines proliferation in a concentration-dependent manner in vitro and potentiate a delay in tumour formation and a decrease in tumour cell proliferation in transgenic OC mouse models (Figure 1) [147]. Studies showed that alendronate, a drug of the bisphosphonates class, reduce stromal invasion, tumour burden, and ascites, suggesting that has anti-tumoral effect in OC [148]. On the other hand, zoledronic acid have an anti-proliferative and anti-invasive activity and presents an interesting potential to delay recurrences in ovarian, endometrial, and breast cancers since, it disturbs relevant steps of tumour dissemination (i.e., invasion and colony formation) [134].
Some reports indicated that bisphosphonates exhibit anti-tumoral properties in many types of cancers, for example, they can inhibit the onset of breast (relative risk (RR) = 0.87; 95% CI = 0.81–0.93) [149] and endometrial (RR = 0.75; 95% CI = 0.60–0.94) [150] cancers. Other epidemiological study reported that bisphosphonates, administrated with or without statins, are associated with a reduced risk of OC [151]. In addition, it was reported that patients bisphosphonates users present a significantly reduced risk for ovarian (OR = 0.49; 95% CI = 0.26–0.93) and endometrial (OR = 0.39; 95% CI = 0.24–0.63) cancers compared to non-users [151].
Hence, it has been shown that bisphosphonates exhibit an anti-tumour effect and a capacity to delay recurrences in the OC setting; however, further studies are needed to evaluate its value as cancer treatment option.
2.4. Ivermectin
Ivermectin, a polycyclic lactone pesticide produced by Streptomyces avermitilis bacterium, is a broad-spectrum antiparasitic agent [152] that binds with high affinity to the glutamic acid operative chloride ion channel localized in nerve and muscle cells in invertebrates [153,154]. This ligation causes increased permeability in the cell membrane to enable chloride ions to enter the cells, resulting in hyperpolarization of nerve and muscle cells, which cause parasite paralysis and extinction [153,154].
Ivermectin is widely used to treat onchocerciasis, lymphatic filariasis, strongyloidiasis, scabies and head lice [155]. In addition, ivermectin can also exhibits other therapeutic actions such as, antibacterial, antiviral and anticancer [156]. As anti-neoplastic agent, it has been demonstrated that ivermectin exhibit anti-tumoral activity in different types of cancers, with emphasis on ovarian, colon and lung cancers, glioma, leukaemia and melanoma [157,158,159,160,161]. Different mechanisms can explain this activity, namely the inhibition of multidrug resistance proteins (MDR), modulation of protein kinase B (Akt)/mTOR and Wnt/T-cell factor (Wnt/TCF) signalling pathways, degradation of p21–activated kinase (PAK-1) and downregulation of stemness genes to preferentially target CSCs populations [158,159,161,162,163,164,165,166,167].
A recent in vitro and in vivo study demonstrated that ivermectin induce cytostatic autophagy in breast cancer cells linked to the inhibition of PAK-1 expression leading to a reduced phosphorylation of Akt and blockage of Akt/mTOR signalling pathway inhibiting tumour growth [163,168]. PAK-1 is abnormally expressed in various neoplasms, including breast, ovarian, pancreatic, colon and prostate cancers and is involved in tumour cell growth and development of chemoresistance [163,166]. Hashimoto et al. demonstrated in vitro that ivermectin induces inactivation of PAK-1 inhibiting OC cells growth [158]. Another recent study demonstrated that ivermectin preferentially targets breast CSCs by increasing the level of intracellular reactive oxygen species (ROS) associated with oxidative stress and DNA damage [161]. In addition, it has been shown that ivermectin could decrease multidrug resistance in breast cancer and enhance the cytotoxicity of doxorubicin and paclitaxel [169]. In glioblastoma cells, ivermectin inhibits angiogenesis and deactivates Akt/mTOR signalling pathway [166]. Moreover, ivermectin significantly inhibits proliferation and induces apoptosis in multiple renal cell carcinoma in vitro, and significantly delays tumour growth in vivo, by induction of mitochondrial dysfunction and oxidative stress [170]. Since ivermectin is a compound that targets yes-associated protein 1 (YAP1) [171], it is anticipated to exhibit anti-tumoral effects against ovarian, gastric, colorectal, and lung cancers, for which high expression of YAP1 is thought to be a prognostic indicator [172,173,174,175,176]. Ivermectin suppress the proliferation of gastric cancer cells in vitro and in vivo via YAP1 expression inhibition in a concentration and time-dependent manner [177]. In chronic myeloid leukaemia, it was demonstrated that ivermectin selectively induces apoptosis by mitochondrial dysfunction and oxidative stress induction [178].
In OC, in vitro and in vivo results show that ivermectin has a karyopherin subunit beta 1 (KPNB1) dependent anti-tumoral effect and the combination of ivermectin and paclitaxel produces a synergistic effect than each drug alone [179]. OC patients with high expression of KPNB1 present poor survival, consequently, ivermectin represents a promising candidate for combinatory treatment in OC. Recently, an interesting study suggest that ivermectin may useful OC combinatory treatments, demonstrating that this drug significantly augmented cisplatin inhibitory effect by suppressing the phosphorylation of key molecules in Akt/mTOR signalling pathway [180]. In same study, using an OC xenograft mouse models, authors showed that ivermectin alone inhibit tumour growth and, in combination with cisplatin, completely reversed tumour growth [180]. Corroborating these findings, another in vivo and vitro study demonstrated that ivermectin reverse the chemoresistance in colorectal, breast, and chronic myeloid leukaemia cancer cells by inhibit epidermal growth factor receptor (EGFR)/extracellular signal-regulated kinases (ERK)/Akt/nuclear factor kappa B (NF-κB) pathway (Figure 1) [181].
Previous findings demonstrate that ivermectin enhances the anti-cancer efficacy of chemotherapeutic drugs, especially in chemoresistant cells. Thus, further studies with ivermectin in combination with chemotherapeutic agents should be performed to validate its use in OC treatment.
2.5. Itraconazole
Itraconazole is a broad-spectrum antifungal agent that inhibits synthesis of ergosterol in the fungal cell membrane by blocking enzyme lanosterol 14a-demethylase, resulting in the destruction of the fungal membrane [182,183,184]. Itraconazole is widely used to treat fungal infections, including aspergillosis, candidiasis, and histoplasmosis, and in immunosuppressive disorders prophylaxis [184,185]. In addition, several experimental and clinical data show promising results regarding itraconazole antiangiogenic activity and has been repurposed as an anti-cancer agent in several types of cancers [184,186,187].
Itraconazole targets different oncobiology mechanisms, including reversing chemoresistance mediated by P-glycoprotein, inhibiting Hedgehog, mTOR, and Wnt/β-catenin signalling pathways, inhibiting angiogenesis and lymphangiogenesis [186,188,189,190,191,192,193,194,195]. A recent study demonstrated that itraconazole is capable of inhibiting mTOR signalling through different upstream mechanisms, e.g., AMPK activation and cholesterol trafficking inhibition that enhances an anti-proliferative and anti-angiogenic effect leading to an increased drug efficacy and reversion of chemoresistance [190]. In addition, an in vitro study showed that itraconazole has anticancer effects on oral squamous cell carcinoma through proteins expression downregulation of Hedgehog pathway by inhibiting cell proliferation and migration [196]. Another in vitro study in pancreatic cancer demonstrated that itraconazole inhibit viability, induce apoptosis and suppress invasion and migration by impaired transforming growth factor beta (TGF-β)/mothers against decapentaplegic homolog 2/3 (SMAD2/3) signalling [197]. In oesophageal cancer, it was demonstrated that itraconazole inhibits cell growth through activating AMPK signalling [198,199].
In the OC setting, a recent study showed a synergistic effect of combining itraconazole and paclitaxel to enhance efficacy in xenograft and patient-derived xenografts (PDX) models derived from OC chemoresistant patients [200]. The authors demonstrated that itraconazole antiangiogenic activity is attributable to its ability to inhibit the vascular endothelial growth factor receptor 2 (VEGFR2) and phosphorylation of ERK, hedgehog, and mTOR pathways (Figure 1) [200]. This study suggests that combining itraconazole and paclitaxel could enhance chemotherapeutic response in epithelial OC patients [200].
Several studies demonstrate that the treatment with itraconazole, in combination with other therapeutic agents, is effective in several types of cancers to increasing the drug efficacy and to overcome chemoresistance [201,202,203,204,205]. In fact, it has been shown that itraconazole can be an effective therapeutic agent for ovarian, breast, prostate, basal cell, non-small-cell lung, endometrial, gastrointestinal, bladder, and pancreatic cancers [186,187,188,202,203,205,206,207,208,209,210,211]. In pancreatic and in non-small-cell lung cancers it has been reported a prolonged survival when itraconazole is administrated as second-line therapy [202,208]. In OC patients unresponsive to platinum agents, the administration of itraconazole combined with taxane-based chemotherapy significantly improved PFS (HR = 0.24; p = 0.002) and overall survival (HR = 0.27; p = 0.006) [203]. Some results demonstrate that itraconazole treatment is beneficial to treat refractory malignancies, including ovarian clear cell, triple-negative breast, pancreatic, and biliary tract cancers [202,203,209,212]. In addition, some preclinical and clinical trial data indicate that itraconazole is capable of reversing the paclitaxel chemoresistance [213,214,215].
Currently, some clinical trials are evaluating the effect of itraconazole as a cancer therapeutic in non-small cell lung cancer (NCT02357836), oesophageal cancer (NCT02749513), basal cell carcinoma (NCT02120677), and OC (Table S1).
Available preclinical and clinical trial data indicate that itraconazole can reverse the paclitaxel chemoresistance. Considering that OC patients frequently present taxane-chemoresistant recurrences, more experimental studies using OC cells are needed to further evaluate this antineoplastic property of this antifungal drug.
2.6. Ritonavir
Ritonavir is a protease inhibitors currently approved for human immunodeficiency virus (HIV) infection treatment to control acquired immune deficiency syndrome (AIDS)) [216]. Highly active anti-retroviral therapy (HAART) is the combination therapy (i.e., reverse transcriptase inhibitors, such as, zidovudine and protease inhibitors, such as, ritonavir and nelfinavir) used to treat patients with HIV infection [217] characterized by an increased risk to develop several types of tumours [217,218,219]. Interestingly, some studies demonstrated that, in HIV patients treated with HAART [220,221,222,223], the incidence rate of some cancers is, in fact, lower. Corroborating these findings, results from other studies reported associations of a potential anti-neoplastic impact of HAART [224,225,226,227]. It has been shown that ritonavir induces apoptosis of lymphoblastic tumour cells including lymphoma, myeloid leukaemia, fibrosarcoma, mastocytoma, and Kaposi’s sarcoma [228,229,230,231]. An in vitro study demonstrated that ritonavir has an effective anti-proliferating activity in OC cells, inducing cell cycle arrest and apoptosis by inhibiting AKT pathway and retinoblastoma phosphorylation [217]. Ritonavir decreases the amount of phosphorylated AKT in a dose-dependent manner, which inhibits the phosphatidylinositol 3-kinase (PI3K)/Akt pathway having anti-tumoral effect (Figure 1). Further results in OC, demonstrate that ritonavir inhibit invasion and migration and has an additive effect when combined with paclitaxel treatment [217].
The evidences on ritonavir action on cancer cell are limited and need further validation. However, these existing data demonstrate that ritonavir has a potential for OC treatment in combination with conventional chemotherapy.
3. Using Ex Vivo Models to Test Individual Drug Repurposing Efficacy
The development of patient-derived cancer cells models to perform drug efficacy tests capable of predicting drug responses constitutes an important step towards a personalized cancer treatment. These tests should consider the phenotype, genotype and protein expression background of each patient tumour to search for effective drugs in accordance to an individual profile of drug response. Determining the chemoresistance profile in each individual patient could facilitate the discovery of the most effective drug for repositioning and treatment could be adapted accordingly [232]. Several ex vivo model systems have been exploited for these purposes: (a) 2D monolayer culture of dissociated cells, including primary cultures and cell lines; (b) 3D tumour cultures, comprising cell lines and organoids; (c) PDX; and (d) organotypic tumour tissue slices. The advantages and disadvantages of each of these systems were reviewed elsewhere [233]. Within these, patient-derived cancer cell culture systems standout, being an easily achievable, non-animal, preclinical model for drug efficacy tests capable of guiding clinical decisions [234]. Indeed, 2D and 3D models may be used for high-throughput drug sensitivity screening, which have started to show promising results with significant higher response rates in patients following guided treatments [235]. Specifically, in epithelial OC, ex vivo models have been shown to faithfully recapitulate phenotypic and genotypic tumour features [236]. Furthermore, results of drug profiling using these OC models showed sensitivity to drugs, such as, platinum and iPARPs, which correlated with patient clinical responses [237]. Likewise, ex vivo models are also suitable for testing high-throughput drug repurposing, as demonstrated in other cancers [238]. In epithelial OC, systematic drug repurposing based on clues from ex vivo testing of human OC patient cells has also began to be explored with case reports of patients showing response to drugs not usually applied [239].
Patient-derived cancer cell models are most commonly established from primary tumours, but can also be derived from metastases, and circulating tumour cells from blood, effusions, or other organic fluids [240]. The choice of tumour samples to be used for drug testing may be crucial to accurately predict patient response over the course of disease with impact in survival. In this respect, epithelial OC constitutes a particular setting given that its primary route of progression is in the peritoneal cavity [241]. Exfoliated tumour cells from the ovary or Fallopian tube are carried by physiological peritoneal fluid and disseminate throughout the abdominal cavity. Extensive peritoneal seeding by tumour cells is often associated with ascites, which may be, detected at the time of diagnosis and more frequently in advanced stages [242]. Malignant ascites comprises a set of cytokines, growth factors, mesothelial cells, macrophages, lymphocytes and tumour cells [243]. The easy accessibility of the peritoneal cavity makes ascites a powerful source of tumour cells, suitable for detecting prognostic and predictive biomarkers, as well as to perform ex vivo assays that could boost the discovery of personalized therapeutic approaches. In the absence of ascites, at diagnosis, tumour tissue for ex-vivo models can be collected simultaneously with sampling for pathology diagnostic purposes. In the setting of recurrence without ascites, biopsy for ex-vivo models should be carefully considered by clinicians together with their patients, as this is an invasive procedure. Establishment of cultures from blood circulating tumour cells, even though challenging, may be an alternative.
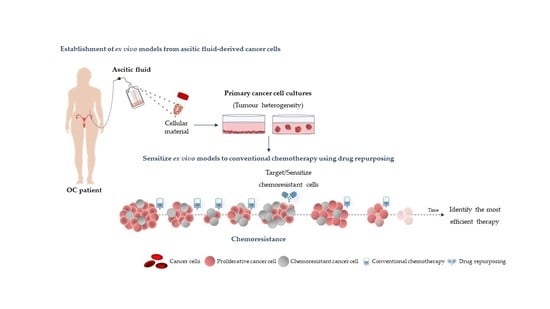
The establishment of ex vivo models from ascitic fluid-derived cancer cells (Figure 2) has been explored as a model to overcome some limitations of strongly manipulated cell lines and potentiate a proof-of-concept for personalized drug efficacy testing [232,234,244,245,246]. One limitation of drug repurposing is the low potency of hit compounds as single agents, as their maximal tolerated dose is often sub therapeutic for cancer treatment purposes [247]. Wisely, combined cocktails using chemotherapeutic drugs and one or more non-oncology drugs can be tested in ascitic fluid-derived cancer cells to deliver an individualized therapeutic solution to OC patients. The drug-repurposing concept aligned to this personalized testing system could further validate the existing evidences supporting the use of these old drugs for cancer treatment.
4. Conclusions
Several researchers worldwide are already investigating recycling the purpose of drugs not originally designed for cancer treatment. These therapies can play an important role in cancer chemoprevention, in recurrence delay, and as partners of old and new therapies, such as chemotherapy. However, this therapeutic strategy faces many obstacles concerning competition with new drug development and patent-related considerations. Many of these difficulties led to the lack of investment by the pharmaceutical industry that impairs the development of research projects that could further validate the current scientific evidences. Drug repurposing will ultimately benefit patients and low-income countries with economical fragile healthcare systems and limited access to new expensive drugs. Thus, off-patent drug research should have a fair financial support to guarantee an accurate result comparison from new and old drugs in cancer settings. Regarding OC, tumour cells present in the ascitic fluid constitute an opportunity to study ex vivo the efficacy of drugs in a personalized manner. This model has great potential to predict the synergistic effect between chemotherapy and repurposing drugs, leading to the best benefit of cancer patients.
Supplementary Materials
The following are available online at https://www.mdpi.com/1422-0067/21/20/7768/s1.
Author Contributions
All of the authors contributed intellectually to the research, drafting, and editing manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This manuscript was funded by HOPE: Improving ovarian cancer patients’ survival—donation from an ovarian cancer patient and by the FCT (Fundação para a Ciência e a Tecnologia) project PTDC/MEC-ONC/29503/2017.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| 2D | Two-dimensional |
| 3D | Three-dimensional |
| AIDS | Acquired immunodeficiency syndrome |
| ADP | Adenosine diphosphate |
| AKT | Protein kinase B |
| AMP | Adenosine monophosphate |
| AMPK | Activated protein kinase |
| ATP | Adenosine triphosphate |
| BRCA | Breast cancer |
| CI | Confidential interval |
| CSCs | Cancer stem cells |
| DNA | Deoxyribonucleic acid |
| EGFR | Epidermal growth factor receptor |
| EMT | Epithelial–mesenchymal transition |
| ERK | Extracellular signal-regulated kinases |
| HAART | Highly active anti-retroviral therapy |
| HGSC | High-grade serous carcinoma |
| HIV | Human immunodeficiency virus |
| HMGCR | 3-Hydroxy-3-methylglutaryl-coenzyme A reductase |
| HR | Hazard ratio |
| iPARPs | PARP inhibitors |
| KPNB1 | Karyopherin subunit beta 1 |
| MDR | Multidrug resistance proteins |
| mTOR | Mammalian target of rapamycin |
| NF-κB | Nuclear factor kappa B |
| OC | Ovarian cancer |
| OD | Odds ratio |
| OS | Overall survival |
| P53/TP53 | Tumour protein |
| PAK-1 | P21–activated kinase |
| PARP | Poly (ADP-ribose) polymerase |
| PDX | Patient derived xenograft |
| PFS | Progression-free survival |
| PI3K | Phosphatidylinositol 3-kinases |
| SMAD2/3 | Mothers against decapentaplegic homolog 2/3 |
| RAS | Rat sarcoma virus |
| ROS | Reactive oxygen species |
| RR | Relative risk |
| TGF-β | Transforming growth factor beta |
| VEGF | Vascular endothelial growth factor |
| VEGFR2 | Vascular endothelial growth factor receptor 2 |
| Wnt/TCF | Wnt/T-cell factor |
| YAP1 | Yes-associated protein 1 |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: Globocan sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.C.M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer Clin. Oncol. 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Ueda, Y.; Naka, T.; Enomoto, T. Therapeutic strategies in epithelial ovarian cancer. J. Exp. Clin. Cancer Res. 2012, 31, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, W.F.; Huang, C.Y.; Chang, M.C.; Hu, Y.H.; Chiang, Y.C.; Chen, Y.L.; Hsieh, C.Y.; Chen, C.A. High mesothelin correlates with chemoresistance and poor survival in epithelial ovarian carcinoma. Br. J. Cancer 2009, 100, 1144–1153. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, C.T.; Fuller, A.F. Intensive surgical and chemotherapeutic management of advanced ovarian cancer. Surg. Clin. N. Am. 1978, 58, 131–142. [Google Scholar] [CrossRef]
- Lheureux, S.; Gourley, C.; Vergote, I.; Oza, A.M. Epithelial ovarian cancer. Lancet 2019, 393, 1240–1253. [Google Scholar] [CrossRef] [Green Version]
- Bowtell, D.D.; Bohm, S.; Ahmed, A.A.; Aspuria, P.J.; Bast, R.C., Jr.; Beral, V.; Berek, J.S.; Birrer, M.J.; Blagden, S.; Bookman, M.A.; et al. Rethinking ovarian cancer ii: Reducing mortality from high-grade serous ovarian cancer. Nat. Rev. Cancer 2015, 15, 668–679. [Google Scholar] [CrossRef]
- Hille, S.; Rein, D.T.; Riffelmann, M.; Neumann, R.; Sartorius, J.; Pfutzner, A.; Kurbacher, C.M.; Schondorf, T.; Breidenbach, M. Anticancer drugs induce mdr1 gene expression in recurrent ovarian cancer. Anticancer Drugs 2006, 17, 1041–1044. [Google Scholar] [CrossRef]
- Howlader, N.N.A.; Krapcho, M.; Miller, D.; Bishop, K.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. (Eds.) Seer Cancer Statistics Review, 1975–2014, National Cancer Institute. Bethesda, md. Available online: Https://seer.Cancer.Gov/csr/1975_2014/ (accessed on 1 August 2020).
- Weidle, U.H.; Birzele, F.; Kollmorgen, G.; Rueger, R. Mechanisms and targets involved in dissemination of ovarian cancer. Cancer Genom. Proteom. 2016, 13, 407–423. [Google Scholar] [CrossRef] [Green Version]
- Aghajanian, C.; Blank, S.V.; Goff, B.A.; Judson, P.L.; Teneriello, M.G.; Husain, A.; Sovak, M.A.; Yi, J.; Nycum, L.R. Oceans: A randomized, double-blind, placebo-controlled phase iii trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J. Clin. Oncol. 2012, 30, 2039–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, R.L.; Brady, M.F.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Walker, J.L.; Kim, B.G.; Fujiwara, K.; Tewari, K.S.; O’Malley, D.M.; et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (nrg oncology/gynecologic oncology group study gog-0213): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 779–791. [Google Scholar] [CrossRef] [Green Version]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.L.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.; Scambia, G.; et al. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ariel3): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 1949–1961. [Google Scholar] [CrossRef] [Green Version]
- Pujade-Lauraine, E.; Ledermann, J.A.; Selle, F.; Gebski, V.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Poveda, A.; Pignata, S.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a brca1/2 mutation (solo2/engot-ov21): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1274–1284. [Google Scholar] [CrossRef] [Green Version]
- Armando, R.G.; Mengual Gomez, D.L.; Gomez, D.E. New drugs are not enoughdrug repositioning in oncology: An update. Int. J. Oncol. 2020, 56, 651–684. [Google Scholar]
- Ashburn, T.T.; Thor, K.B. Drug repositioning: Identifying and developing new uses for existing drugs. Nat. Rev. Drug Discov. 2004, 3, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, F.; Sukhatme, V.P.; Bouche, G. Drug repurposing in oncology--patient and health systems opportunities. Nat. Rev. Clin. Oncol. 2015, 12, 732–742. [Google Scholar] [CrossRef]
- Nowak-Sliwinska, P.; Scapozza, L.; Ruiz, I.A.A. Drug repurposing in oncology: Compounds, pathways, phenotypes and computational approaches for colorectal cancer. Biochim. Biophys. Acta Rev. Cancer 2019, 1871, 434–454. [Google Scholar] [CrossRef]
- Gunjan, S.; Sharma, T.; Yadav, K.; Chauhan, B.S.; Singh, S.K.; Siddiqi, M.I.; Tripathi, R. Artemisinin derivatives and synthetic trioxane trigger apoptotic cell death in asexual stages of plasmodium. Front. Cell Infect. Microbiol. 2018, 8, 256. [Google Scholar] [CrossRef]
- Goldstein, J.L.; Brown, M.S. Regulation of the mevalonate pathway. Nature 1990, 343, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Kaitin, K.I.; DiMasi, J.A. Pharmaceutical innovation in the 21st century: New drug approvals in the first decade, 2000–2009. Clin. Pharmacol. Ther. 2011, 89, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Schachter, M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: An update. Fundam. Clin. Pharmacol. 2005, 19, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Padhy, B.M.; Gupta, Y.K. Drug repositioning: Re-investigating existing drugs for new therapeutic indications. J. Postgrad. Med. 2011, 57, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Akinwunmi, B.; Vitonis, A.F.; Titus, L.; Terry, K.L.; Cramer, D.W. Statin therapy and association with ovarian cancer risk in the new england case control (nec) study. Int. J. Cancer 2019, 144, 991–1000. [Google Scholar] [CrossRef]
- Davies, J.T.; Delfino, S.F.; Feinberg, C.E.; Johnson, M.F.; Nappi, V.L.; Olinger, J.T.; Schwab, A.P.; Swanson, H.I. Current and emerging uses of statins in clinical therapeutics: A review. Lipid Insights 2016, 9, 13–29. [Google Scholar] [CrossRef] [Green Version]
- Knickelbine, T.; Lui, M.; Garberich, R.; Miedema, M.D.; Strauss, C.; VanWormer, J.J. Familial hypercholesterolemia in a large ambulatory population: Statin use, optimal treatment, and identification for advanced medical therapies. J. Clin. Lipidol. 2016, 10, 1182–1187. [Google Scholar] [CrossRef]
- Pletcher, M.J.; Pignone, M.; Jarmul, J.A.; Moran, A.E.; Vittinghoff, E.; Newman, T. Population impact & efficiency of benefit-targeted versus risk-targeted statin prescribing for primary prevention of cardiovascular disease. J. Am. Heart Assoc. 2017, 6, e004316. [Google Scholar]
- Fernandez-Sauze, S.; Grall, D.; Cseh, B.; Van Obberghen-Schilling, E. Regulation of fibronectin matrix assembly and capillary morphogenesis in endothelial cells by rho family gtpases. Exp. Cell Res. 2009, 315, 2092–2104. [Google Scholar] [CrossRef]
- Mizuno, Y.; Jacob, R.F.; Mason, R.P. Inflammation and the development of atherosclerosis. J. Atheroscler. Thromb. 2011, 18, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Spuul, P.; Ciufici, P.; Veillat, V.; Leclercq, A.; Daubon, T.; Kramer, I.J.; Genot, E. Importance of rhogtpases in formation, characteristics, and functions of invadosomes. Small GTPases 2014, 5, e28195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeybek, B.; Costantine, M.; Kilic, G.S.; Borahay, M.A. Therapeutic roles of statins in gynecology and obstetrics: The current evidence. Reprod. Sci. 2018, 25, 802–817. [Google Scholar] [CrossRef] [PubMed]
- Clendening, J.W.; Pandyra, A.; Boutros, P.C.; El Ghamrasni, S.; Khosravi, F.; Trentin, G.A.; Martirosyan, A.; Hakem, A.; Hakem, R.; Jurisica, I.; et al. Dysregulation of the mevalonate pathway promotes transformation. Proc. Natl. Acad. Sci. USA 2010, 107, 15051–15056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martirosyan, A.; Clendening, J.W.; Goard, C.A.; Penn, L.Z. Lovastatin induces apoptosis of ovarian cancer cells and synergizes with doxorubicin: Potential therapeutic relevance. BMC Cancer 2010, 10, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, E.; Nandi, M.; Wilkinson, L.L.; Arrowsmith, D.M.; Curtis, A.D.; Richardson, A. Preclinical evaluation of statins as a treatment for ovarian cancer. Gynecol. Oncol. 2013, 129, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.W.; Dimitroulakos, J.; Minden, M.D.; Penn, L.Z. Hmg-coa reductase inhibitors and the malignant cell: The statin family of drugs as triggers of tumor-specific apoptosis. Leukemia 2002, 16, 508–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, H.M.; Fang, Z.; Sun, W.; Clark, L.H.; Stine, J.E.; Tran, A.Q.; Sullivan, S.A.; Gilliam, T.P.; Zhou, C.; Bae-Jump, V.L. Atorvastatin exhibits anti-tumorigenic and anti-metastatic effects in ovarian cancer in vitro. Am. J. Cancer Res. 2017, 7, 2478–2490. [Google Scholar]
- Pich, C.; Teiti, I.; Rochaix, P.; Mariame, B.; Couderc, B.; Favre, G.; Tilkin-Mariame, A.F. Statins reduce melanoma development and metastasis through mica overexpression. Front. Immunol. 2013, 4, 62. [Google Scholar] [CrossRef] [Green Version]
- Kidera, Y.; Tsubaki, M.; Yamazoe, Y.; Shoji, K.; Nakamura, H.; Ogaki, M.; Satou, T.; Itoh, T.; Isozaki, M.; Kaneko, J.; et al. Reduction of lung metastasis, cell invasion, and adhesion in mouse melanoma by statin-induced blockade of the rho/rho-associated coiled-coil-containing protein kinase pathway. J. Exp. Clin. Cancer Res. 2010, 29, 127. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Wang, Z.; Li, Y.; Li, W.; Chen, Y. Simvastatin prevents proliferation and bone metastases of lung adenocarcinoma in vitro and in vivo. Neoplasma 2013, 60, 240–246. [Google Scholar] [CrossRef]
- Yu, X.; Luo, Y.; Zhou, Y.; Zhang, Q.; Wang, J.; Wei, N.; Mi, M.; Zhu, J.; Wang, B.; Chang, H.; et al. Brca1 overexpression sensitizes cancer cells to lovastatin via regulation of cyclin d1-cdk4-p21waf1/cip1 pathway: Analyses using a breast cancer cell line and tumoral xenograft model. Int. J. Oncol. 2008, 33, 555–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Z.; Fan-Minogue, H.; Bellovin, D.I.; Yevtodiyenko, A.; Arzeno, J.; Yang, Q.; Gambhir, S.S.; Felsher, D.W. Myc phosphorylation, activation, and tumorigenic potential in hepatocellular carcinoma are regulated by hmg-coa reductase. Cancer Res. 2011, 71, 2286–2297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sassano, A.; Platanias, L.C. Statins in tumor suppression. Cancer Lett. 2008, 260, 11–19. [Google Scholar] [CrossRef]
- Greenaway, J.B.; Virtanen, C.; Osz, K.; Revay, T.; Hardy, D.; Shepherd, T.; DiMattia, G.; Petrik, J. Ovarian tumour growth is characterized by mevalonate pathway gene signature in an orthotopic, syngeneic model of epithelial ovarian cancer. Oncotarget 2016, 7, 47343–47365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, Y.; Kashima, H.; Wu, R.C.; Jung, J.G.; Kuan, J.C.; Gu, J.; Xuan, J.; Sokoll, L.; Visvanathan, K.; Shih Ie, M.; et al. Mevalonate pathway antagonist suppresses formation of serous tubal intraepithelial carcinoma and ovarian carcinoma in mouse models. Clin. Cancer Res. 2015, 21, 4652–4662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stine, J.E.; Guo, H.; Sheng, X.; Han, X.; Schointuch, M.N.; Gilliam, T.P.; Gehrig, P.A.; Zhou, C.; Bae-Jump, V.L. The hmg-coa reductase inhibitor, simvastatin, exhibits anti-metastatic and anti-tumorigenic effects in ovarian cancer. Oncotarget 2016, 7, 946–960. [Google Scholar] [CrossRef]
- Cuello, F.M.; Kato, S.C.; Díaz, S.D.; Owen, G. Effects of statins in cancer. Rev. Med. Chil. 2013, 141, 227–236. [Google Scholar]
- Laezza, C.; Malfitano, A.M.; Proto, M.C.; Esposito, I.; Gazzerro, P.; Formisano, P.; Pisanti, S.; Santoro, A.; Caruso, M.G.; Bifulco, M. Inhibition of 3-hydroxy-3-methylglutaryl-coenzyme a reductase activity and of ras farnesylation mediate antitumor effects of anandamide in human breast cancer cells. Endocr. Relat. Cancer 2010, 17, 495–503. [Google Scholar] [CrossRef]
- Horiuchi, A.; Kikuchi, N.; Osada, R.; Wang, C.; Hayashi, A.; Nikaido, T.; Konishi, I. Overexpression of rhoa enhances peritoneal dissemination: Rhoa suppression with lovastatin may be useful for ovarian cancer. Cancer Sci. 2008, 99, 2532–2539. [Google Scholar] [CrossRef]
- Liu, H.; Liang, S.L.; Kumar, S.; Weyman, C.M.; Liu, W.; Zhou, A. Statins induce apoptosis in ovarian cancer cells through activation of jnk and enhancement of bim expression. Cancer Chemother. Pharmacol. 2009, 63, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Matsuura, M.; Suzuki, T.; Suzuki, M.; Tanaka, R.; Ito, E.; Saito, T. Statin-mediated reduction of osteopontin expression induces apoptosis and cell growth arrest in ovarian clear cell carcinoma. Oncol. Rep. 2011, 25, 41–47. [Google Scholar] [CrossRef] [PubMed]
- de Wolf, E.; Abdullah, M.I.; Jones, S.M.; Menezes, K.; Moss, D.M.; Drijfhout, F.P.; Hart, S.R.; Hoskins, C.; Stronach, E.A.; Richardson, A. Dietary geranylgeraniol can limit the activity of pitavastatin as a potential treatment for drug-resistant ovarian cancer. Sci. Rep. 2017, 7, 5410. [Google Scholar] [CrossRef] [PubMed]
- Bischof, K.; Knappskog, S.; Hjelle, S.M.; Stefansson, I.; Woie, K.; Salvesen, H.B.; Gjertsen, B.T.; Bjorge, L. Influence of p53 isoform expression on survival in high-grade serous ovarian cancers. Sci. Rep. 2019, 9, 5244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandoth, C.; McLellan, M.D.; Vandin, F.; Ye, K.; Niu, B.; Lu, C.; Xie, M.; Zhang, Q.; McMichael, J.F.; Wyczalkowski, M.A.; et al. Mutational landscape and significance across 12 major cancer types. Nature 2013, 502, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Patch, A.M.; Christie, E.L.; Etemadmoghadam, D.; Garsed, D.W.; George, J.; Fereday, S.; Nones, K.; Cowin, P.; Alsop, K.; Bailey, P.J.; et al. Whole-genome characterization of chemoresistant ovarian cancer. Nature 2015, 521, 489–494. [Google Scholar] [CrossRef]
- Brennan, D.J.; Brandstedt, J.; Rexhepaj, E.; Foley, M.; Ponten, F.; Uhlen, M.; Gallagher, W.M.; O’Connor, D.P.; O’Herlihy, C.; Jirstrom, K. Tumour-specific hmg-coar is an independent predictor of recurrence free survival in epithelial ovarian cancer. BMC Cancer 2010, 10, 125. [Google Scholar] [CrossRef] [Green Version]
- Xie, W.; Ning, L.; Huang, Y.; Liu, Y.; Zhang, W.; Hu, Y.; Lang, J.; Yang, J. Statin use and survival outcomes in endocrine-related gynecologic cancers: A systematic review and meta-analysis. Oncotarget 2017, 8, 41508–41517. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Zhou, J. Impact of postdiagnostic statin use on ovarian cancer mortality: A systematic review and meta-analysis of observational studies. Br. J. Clin. Pharmacol. 2018, 84, 1109–1120. [Google Scholar] [CrossRef] [Green Version]
- Urpilainen, E.; Marttila, M.; Hautakoski, A.; Arffman, M.; Sund, R.; Ilanne-Parikka, P.; Arima, R.; Kangaskokko, J.; Puistola, U.; Laara, E.; et al. The role of metformin and statins in the incidence of epithelial ovarian cancer in type 2 diabetes: A cohort and nested case-control study. BJOG 2018, 125, 1001–1008. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, S.F.; Nordestgaard, B.G.; Bojesen, S.E. Statin use and reduced cancer-related mortality. N. Engl. J. Med. 2012, 367, 1792–1802. [Google Scholar] [CrossRef] [Green Version]
- Couttenier, A.; Lacroix, O.; Vaes, E.; Cardwell, C.R.; De Schutter, H.; Robert, A. Statin use is associated with improved survival in ovarian cancer: A retrospective population-based study. PLoS ONE 2017, 12, e0189233. [Google Scholar] [CrossRef] [PubMed]
- Graaf, M.R.; Beiderbeck, A.B.; Egberts, A.C.; Richel, D.J.; Guchelaar, H.J. The risk of cancer in users of statins. J. Clin. Oncol. 2004, 22, 2388–2394. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Murphy, L.; Zgaga, L.; Barron, T.I.; Bennett, K. Pre-diagnostic statin use, lymph node status and mortality in women with stages i-iii breast cancer. Br. J. Cancer 2017, 117, 588–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardwell, C.R.; Hicks, B.M.; Hughes, C.; Murray, L.J. Statin use after colorectal cancer diagnosis and survival: A population-based cohort study. J. Clin. Oncol. 2014, 32, 3177–3183. [Google Scholar] [CrossRef]
- Yu, O.; Eberg, M.; Benayoun, S.; Aprikian, A.; Batist, G.; Suissa, S.; Azoulay, L. Use of statins and the risk of death in patients with prostate cancer. J. Clin. Oncol. 2014, 32, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Vogel, T.J.; Goodman, M.T.; Li, A.J.; Jeon, C.Y. Statin treatment is associated with survival in a nationally representative population of elderly women with epithelial ovarian cancer. Gynecol. Oncol. 2017, 146, 340–345. [Google Scholar] [CrossRef]
- Knox, J.J.; Siu, L.L.; Chen, E.; Dimitroulakos, J.; Kamel-Reid, S.; Moore, M.J.; Chin, S.; Irish, J.; LaFramboise, S.; Oza, A.M. A phase i trial of prolonged administration of lovastatin in patients with recurrent or metastatic squamous cell carcinoma of the head and neck or of the cervix. Eur. J. Cancer 2005, 41, 523–530. [Google Scholar] [CrossRef]
- Kornblau, S.M.; Banker, D.E.; Stirewalt, D.; Shen, D.; Lemker, E.; Verstovsek, S.; Estrov, Z.; Faderl, S.; Cortes, J.; Beran, M.; et al. Blockade of adaptive defensive changes in cholesterol uptake and synthesis in aml by the addition of pravastatin to idarubicin + high-dose ara-c: A phase 1 study. Blood 2007, 109, 2999–3006. [Google Scholar] [CrossRef]
- Minden, M.D.; Dimitroulakos, J.; Nohynek, D.; Penn, L.Z. Lovastatin induced control of blast cell growth in an elderly patient with acute myeloblastic leukemia. Leuk. Lymphoma 2001, 40, 659–662. [Google Scholar] [CrossRef]
- Schmidmaier, R.; Baumann, P.; Bumeder, I.; Meinhardt, G.; Straka, C.; Emmerich, B. First clinical experience with simvastatin to overcome drug resistance in refractory multiple myeloma. Eur. J. Haematol. 2007, 79, 240–243. [Google Scholar] [CrossRef]
- Van der Spek, E.; Bloem, A.C.; van de Donk, N.W.; Bogers, L.H.; van der Griend, R.; Kramer, M.H.; de Weerdt, O.; Wittebol, S.; Lokhorst, H.M. Dose-finding study of high-dose simvastatin combined with standard chemotherapy in patients with relapsed or refractory myeloma or lymphoma. Haematologica 2006, 91, 542–545. [Google Scholar] [PubMed]
- Cusi, K.; Consoli, A.; DeFronzo, R.A. Metabolic effects of metformin on glucose and lactate metabolism in noninsulin-dependent diabetes mellitus. J. Clin. Endocrinol. Metab. 1996, 81, 4059–4067. [Google Scholar] [PubMed] [Green Version]
- Mues, C.; Zhou, J.; Manolopoulos, K.N.; Korsten, P.; Schmoll, D.; Klotz, L.O.; Bornstein, S.R.; Klein, H.H.; Barthel, A. Regulation of glucose-6-phosphatase gene expression by insulin and metformin. Horm. Metab. Res. 2009, 41, 730–735. [Google Scholar] [CrossRef]
- Stephenne, X.; Foretz, M.; Taleux, N.; van der Zon, G.C.; Sokal, E.; Hue, L.; Viollet, B.; Guigas, B. Metformin activates amp-activated protein kinase in primary human hepatocytes by decreasing cellular energy status. Diabetologia 2011, 54, 3101–3110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viollet, B.; Guigas, B.; Sanz Garcia, N.; Leclerc, J.; Foretz, M.; Andreelli, F. Cellular and molecular mechanisms of metformin: An overview. Clin. Sci. 2012, 122, 253–270. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.O.; Lee, S.K.; Kim, J.H.; Kim, N.; You, G.Y.; Moon, J.W.; Kim, S.J.; Park, S.H.; Kim, H.S. Metformin regulates glucose transporter 4 (glut4) translocation through amp-activated protein kinase (ampk)-mediated cbl/cap signaling in 3t3-l1 preadipocyte cells. J. Biol. Chem. 2012, 287, 44121–44129. [Google Scholar] [CrossRef] [Green Version]
- Wheaton, W.W.; Weinberg, S.E.; Hamanaka, R.B.; Soberanes, S.; Sullivan, L.B.; Anso, E.; Glasauer, A.; Dufour, E.; Mutlu, G.M.; Budigner, G.S.; et al. Metformin inhibits mitochondrial complex i of cancer cells to reduce tumorigenesis. Elife 2014, 3, e02242. [Google Scholar] [CrossRef]
- Pernicova, I.; Korbonits, M. Metformin--mode of action and clinical implications for diabetes and cancer. Nat. Rev. Endocrinol. 2014, 10, 143–156. [Google Scholar] [CrossRef]
- Pollak, M. The insulin and insulin-like growth factor receptor family in neoplasia: An update. Nat. Rev. Cancer 2012, 12, 159–169. [Google Scholar] [CrossRef]
- Pollak, M.N. Investigating metformin for cancer prevention and treatment: The end of the beginning. Cancer Discov. 2012, 2, 778–790. [Google Scholar] [CrossRef] [Green Version]
- Moiseeva, O.; Deschenes-Simard, X.; Pollak, M.; Ferbeyre, G. Metformin, aging and cancer. Aging Albany NY 2013, 5, 330–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, E.L.; Walsh, M.C.; Cejas, P.J.; Harms, G.M.; Shen, H.; Wang, L.S.; Jones, R.G.; Choi, Y. Enhancing cd8 t-cell memory by modulating fatty acid metabolism. Nature 2009, 460, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; Bardeesy, N.; Manning, B.D.; Lopez, L.; Kosmatka, M.; DePinho, R.A.; Cantley, L.C. The lkb1 tumor suppressor negatively regulates mtor signaling. Cancer Cell 2004, 6, 91–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakikhani, M.; Dowling, R.J.; Sonenberg, N.; Pollak, M.N. The effects of adiponectin and metformin on prostate and colon neoplasia involve activation of amp-activated protein kinase. Cancer Prev. Res. 2008, 1, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Lengyel, E.; Litchfield, L.M.; Mitra, A.K.; Nieman, K.M.; Mukherjee, A.; Zhang, Y.; Johnson, A.; Bradaric, M.; Lee, W.; Romero, I.L. Metformin inhibits ovarian cancer growth and increases sensitivity to paclitaxel in mouse models. Am. J. Obstet. Gynecol. 2015, 212, 479.e1–479.e10. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Romero, I.L.; Litchfield, L.M.; Lengyel, E.; Locasale, J.W. Metformin targets central carbon metabolism and reveals mitochondrial requirements in human cancers. Cell Metab. 2016, 24, 728–739. [Google Scholar] [CrossRef]
- Gui, D.Y.; Sullivan, L.B.; Luengo, A.; Hosios, A.M.; Bush, L.N.; Gitego, N.; Davidson, S.M.; Freinkman, E.; Thomas, C.J.; Vander Heiden, M.G. Environment dictates dependence on mitochondrial complex i for nad+ and aspartate production and determines cancer cell sensitivity to metformin. Cell Metab. 2016, 24, 716–727. [Google Scholar] [CrossRef] [Green Version]
- Kurelac, I.; Umesh Ganesh, N.; Iorio, M.; Porcelli, A.M.; Gasparre, G. The multifaceted effects of metformin on tumor microenvironment. Semin. Cell Dev. Biol. 2020, 98, 90–97. [Google Scholar] [CrossRef]
- Li, X.; Li, B.; Ni, Z.; Zhou, P.; Wang, B.; He, J.; Xiong, H.; Yang, F.; Wu, Y.; Lyu, X.; et al. Metformin synergizes with bcl-xl/bcl-2 inhibitor abt-263 to induce apoptosis specifically in p53-defective cancer cells. Mol. Cancer Ther. 2017, 16, 1806–1818. [Google Scholar] [CrossRef] [Green Version]
- Galdieri, L.; Gatla, H.; Vancurova, I.; Vancura, A. Activation of amp-activated protein kinase by metformin induces protein acetylation in prostate and ovarian cancer cells. J. Biol. Chem. 2016, 291, 25154–25166. [Google Scholar] [CrossRef] [Green Version]
- Rattan, R.; Giri, S.; Hartmann, L.C.; Shridhar, V. Metformin attenuates ovarian cancer cell growth in an amp-kinase dispensable manner. J. Cell. Mol. Med. 2011, 15, 166–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Y.; Peng, Z.; Shi, M.; Ji, M.; Guo, H.; Shi, H. Metformin combined with p38 mapk inhibitor improves cisplatin sensitivity in cisplatinresistant ovarian cancer. Mol. Med. Rep. 2014, 10, 2346–2350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Zhang, P.; Wang, H.; Hou, D.; Li, W.; Xiao, G.; Li, C. Inhibitory effects of metformin at low concentration on epithelial-mesenchymal transition of cd44(+)cd117(+) ovarian cancer stem cells. Stem Cell. Res. Ther. 2015, 6, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.; Zhao, N.; Li, D.; Zou, G.; Chen, Y. Metformin improves the sensitivity of ovarian cancer cells to chemotherapeutic agents. Oncol. Lett. 2019, 18, 2404–2411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, J.; Shi, H.R.; Ren, F.; Wang, J.L.; Wu, Q.H.; Li, X.; Zhang, R.T. Inhibition of the igf signaling pathway reverses cisplatin resistance in ovarian cancer cells. BMC Cancer 2017, 17, 851. [Google Scholar] [CrossRef]
- Gotlieb, W.H.; Saumet, J.; Beauchamp, M.C.; Gu, J.; Lau, S.; Pollak, M.N.; Bruchim, I. In vitro metformin anti-neoplastic activity in epithelial ovarian cancer. Gynecol. Oncol. 2008, 110, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Feng, Y.; Liu, H.; Wu, J.; Tang, Y.; Wang, Q. Real-time assessment of platinum sensitivity of primary culture from a patient with ovarian cancer with extensive metastasis and the platinum sensitivity enhancing effect by metformin. Oncol. Lett. 2018, 16, 4253–4262. [Google Scholar] [CrossRef] [Green Version]
- Rattan, R.; Graham, R.P.; Maguire, J.L.; Giri, S.; Shridhar, V. Metformin suppresses ovarian cancer growth and metastasis with enhancement of cisplatin cytotoxicity in vivo. Neoplasia 2011, 13, 483–491. [Google Scholar] [CrossRef] [Green Version]
- Wu, B.; Li, S.; Sheng, L.; Zhu, J.; Gu, L.; Shen, H.; La, D.; Hambly, B.D.; Bao, S.; Di, W. Metformin inhibits the development and metastasis of ovarian cancer. Oncol. Rep. 2012, 28, 903–908. [Google Scholar] [CrossRef] [Green Version]
- Yasmeen, A.; Beauchamp, M.C.; Piura, E.; Segal, E.; Pollak, M.; Gotlieb, W.H. Induction of apoptosis by metformin in epithelial ovarian cancer: Involvement of the bcl-2 family proteins. Gynecol. Oncol. 2011, 121, 492–498. [Google Scholar] [CrossRef]
- Patel, S.; Kumar, L.; Singh, N. Metformin and epithelial ovarian cancer therapeutics. Cell. Oncol. 2015, 38, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Shank, J.J.; Yang, K.; Ghannam, J.; Cabrera, L.; Johnston, C.J.; Reynolds, R.K.; Buckanovich, R.J. Metformin targets ovarian cancer stem cells in vitro and in vivo. Gynecol. Oncol. 2012, 127, 390–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dang, J.H.; Jin, Z.J.; Liu, X.J.; Hu, D.; Wang, J.; Luo, Y.; Li, L.L. Metformin in combination with cisplatin inhibits cell viability and induces apoptosis of human ovarian cancer cells by inactivating erk 1/2. Oncol. Lett. 2017, 14, 7557–7564. [Google Scholar] [CrossRef] [Green Version]
- Hijaz, M.; Chhina, J.; Mert, I.; Taylor, M.; Dar, S.; Al-Wahab, Z.; Ali-Fehmi, R.; Buekers, T.; Munkarah, A.R.; Rattan, R. Preclinical evaluation of olaparib and metformin combination in brca1 wildtype ovarian cancer. Gynecol. Oncol. 2016, 142, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Franciosi, M.; Lucisano, G.; Lapice, E.; Strippoli, G.F.; Pellegrini, F.; Nicolucci, A. Metformin therapy and risk of cancer in patients with type 2 diabetes: Systematic review. PLoS ONE 2013, 8, e71583. [Google Scholar] [CrossRef]
- Noto, H.; Goto, A.; Tsujimoto, T.; Noda, M. Cancer risk in diabetic patients treated with metformin: A systematic review and meta-analysis. PLoS ONE 2012, 7, e33411. [Google Scholar] [CrossRef]
- Chu, D.; Wu, J.; Wang, K.; Zhao, M.; Wang, C.; Li, L.; Guo, R. Effect of metformin use on the risk and prognosis of endometrial cancer: A systematic review and meta-analysis. BMC Cancer 2018, 18, 438. [Google Scholar] [CrossRef] [Green Version]
- Hanna, R.K.; Zhou, C.; Malloy, K.M.; Sun, L.; Zhong, Y.; Gehrig, P.A.; Bae-Jump, V.L. Metformin potentiates the effects of paclitaxel in endometrial cancer cells through inhibition of cell proliferation and modulation of the mtor pathway. Gynecol. Oncol. 2012, 125, 458–469. [Google Scholar] [CrossRef] [Green Version]
- Bodmer, M.; Becker, C.; Meier, C.; Jick, S.S.; Meier, C.R. Use of metformin and the risk of ovarian cancer: A case-control analysis. Gynecol. Oncol. 2011, 123, 200–204. [Google Scholar] [CrossRef]
- Dilokthornsakul, P.; Chaiyakunapruk, N.; Termrungruanglert, W.; Pratoomsoot, C.; Saokaew, S.; Sruamsiri, R. The effects of metformin on ovarian cancer: A systematic review. Int. J. Gynecol. Cancer 2013, 23, 1544–1551. [Google Scholar] [CrossRef]
- Romero, I.L.; McCormick, A.; McEwen, K.A.; Park, S.; Karrison, T.; Yamada, S.D.; Pannain, S.; Lengyel, E. Relationship of type ii diabetes and metformin use to ovarian cancer progression, survival, and chemosensitivity. Obstet. Gynecol. 2012, 119, 61–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, J.; Liu, B.; Wang, H.; Zhang, T.; Yang, L. Association of metformin use with ovarian cancer incidence and prognosis: A systematic review and meta-analysis. Int. J. Gynecol. Cancer 2019, 29, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.B.; Lei, K.J.; Liu, J.P.; Jia, Y.M. Continuous use of metformin can improve survival in type 2 diabetic patients with ovarian cancer: A retrospective study. Medicine 2017, 96, e7605. [Google Scholar] [CrossRef]
- Kumar, S.; Meuter, A.; Thapa, P.; Langstraat, C.; Giri, S.; Chien, J.; Rattan, R.; Cliby, W.; Shridhar, V. Metformin intake is associated with better survival in ovarian cancer: A case-control study. Cancer 2013, 119, 555–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.J.; Li, S. The prognostic value of metformin for cancer patients with concurrent diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2014, 16, 707–710. [Google Scholar] [CrossRef]
- Gong, T.T.; Wu, Q.J.; Lin, B.; Ruan, S.K.; Kushima, M.; Takimoto, M. Observational studies on the association between post-diagnostic metformin use and survival in ovarian cancer: A systematic review and meta-analysis. Front. Oncol. 2019, 9, 458. [Google Scholar] [CrossRef]
- Evans, J.M.; Donnelly, L.A.; Emslie-Smith, A.M.; Alessi, D.R.; Morris, A.D. Metformin and reduced risk of cancer in diabetic patients. BMJ 2005, 330, 1304–1305. [Google Scholar] [CrossRef] [Green Version]
- Gandini, S.; Puntoni, M.; Heckman-Stoddard, B.M.; Dunn, B.K.; Ford, L.; DeCensi, A.; Szabo, E. Metformin and cancer risk and mortality: A systematic review and meta-analysis taking into account biases and confounders. Cancer Prev. Res. 2014, 7, 867–885. [Google Scholar] [CrossRef] [Green Version]
- Saraei, P.; Asadi, I.; Kakar, M.A.; Moradi-Kor, N. The beneficial effects of metformin on cancer prevention and therapy: A comprehensive review of recent advances. Cancer Manag. Res. 2019, 11, 3295–3313. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Zhong, X.; Gao, P.; Shi, J.; Wu, Z.; Guo, Z.; Wang, Z.; Song, Y. The potential effect of metformin on cancer: An umbrella review. Front. Endocrinol. 2019, 10, 617. [Google Scholar] [CrossRef]
- Zi, F.; Zi, H.; Li, Y.; He, J.; Shi, Q.; Cai, Z. Metformin and cancer: An existing drug for cancer prevention and therapy. Oncol. Lett. 2018, 15, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Bao, B.; Azmi, A.S.; Ali, S.; Zaiem, F.; Sarkar, F.H. Metformin may function as anti-cancer agent via targeting cancer stem cells: The potential biological significance of tumor-associated mirnas in breast and pancreatic cancers. Ann. Transl. Med. 2014, 2, 59. [Google Scholar] [PubMed]
- Chae, J.W.; Baek, I.H.; Lee, B.Y.; Cho, S.K.; Kwon, K.I. Population pk/pd analysis of metformin using the signal transduction model. Br. J. Clin. Pharmacol. 2012, 74, 815–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shackelford, D.B.; Abt, E.; Gerken, L.; Vasquez, D.S.; Seki, A.; Leblanc, M.; Wei, L.; Fishbein, M.C.; Czernin, J.; Mischel, P.S.; et al. Lkb1 inactivation dictates therapeutic response of non-small cell lung cancer to the metabolism drug phenformin. Cancer Cell 2013, 23, 143–158. [Google Scholar] [CrossRef] [Green Version]
- Pierotti, M.A.; Berrino, F.; Gariboldi, M.; Melani, C.; Mogavero, A.; Negri, T.; Pasanisi, P.; Pilotti, S. Targeting metabolism for cancer treatment and prevention: Metformin, an old drug with multi-faceted effects. Oncogene 2013, 32, 1475–1487. [Google Scholar] [CrossRef] [PubMed]
- Eikawa, S.; Nishida, M.; Mizukami, S.; Yamazaki, C.; Nakayama, E.; Udono, H. Immune-mediated antitumor effect by type 2 diabetes drug, metformin. Proc. Natl. Acad. Sci. USA 2015, 112, 1809–1814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Barco, S.; Vazquez-Martin, A.; Cufi, S.; Oliveras-Ferraros, C.; Bosch-Barrera, J.; Joven, J.; Martin-Castillo, B.; Menendez, J.A. Metformin: Multi-faceted protection against cancer. Oncotarget 2011, 2, 896–917. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.R.; Chan, D.K.; Shank, J.J.; Griffith, K.A.; Fan, H.; Szulawski, R.; Yang, K.; Reynolds, R.K.; Johnston, C.; McLean, K.; et al. Phase ii clinical trial of metformin as a cancer stem cell-targeting agent in ovarian cancer. JCI Insight 2020, 5, e133247. [Google Scholar]
- Broekman, K.E.; Hof, M.A.J.; Touw, D.J.; Gietema, J.A.; Nijman, H.W.; Lefrandt, J.D.; Reyners, A.K.L.; Jalving, M. Phase i study of metformin in combination with carboplatin/paclitaxel chemotherapy in patients with advanced epithelial ovarian cancer. Invest. New Drugs 2020, 38, 1454–1462. [Google Scholar] [CrossRef] [Green Version]
- Mystakidou, K.; Katsouda, E.; Stathopoulou, E.; Vlahos, L. Approaches to managing bone metastases from breast cancer: The role of bisphosphonates. Cancer Treat. Rev. 2005, 31, 303–311. [Google Scholar] [CrossRef]
- Russell, R.G.; Rogers, M.J. Bisphosphonates: From the laboratory to the clinic and back again. Bone 1999, 25, 97–106. [Google Scholar] [CrossRef]
- Gronich, N.; Rennert, G. Beyond aspirin-cancer prevention with statins, metformin and bisphosphonates. Nat. Rev. Clin. Oncol. 2013, 10, 625–642. [Google Scholar] [CrossRef] [PubMed]
- Muinelo-Romay, L.; Garcia, D.; Alonso-Alconada, L.; Vieito, M.; Carmona, M.; Martinez, N.; Aguin, S.; Abal, M.; Lopez-Lopez, R. Zoledronic acid as an antimetastatic agent for different human tumor cell lines. Anticancer Res. 2013, 33, 5295–5300. [Google Scholar] [PubMed]
- Yuasa, T.; Kimura, S.; Ashihara, E.; Habuchi, T.; Maekawa, T. Zoledronic acid-a multiplicity of anti-cancer action. Curr. Med. Chem. 2007, 14, 2126–2135. [Google Scholar] [CrossRef] [PubMed]
- Gnant, M.; Mlineritsch, B.; Schippinger, W.; Luschin-Ebengreuth, G.; Postlberger, S.; Menzel, C.; Jakesz, R.; Seifert, M.; Hubalek, M.; Bjelic-Radisic, V.; et al. Endocrine therapy plus zoledronic acid in premenopausal breast cancer. N. Engl. J. Med. 2009, 360, 679–691. [Google Scholar] [CrossRef]
- Coleman, R.E.; Winter, M.C.; Cameron, D.; Bell, R.; Dodwell, D.; Keane, M.M.; Gil, M.; Ritchie, D.; Passos-Coelho, J.L.; Wheatley, D.; et al. The effects of adding zoledronic acid to neoadjuvant chemotherapy on tumour response: Exploratory evidence for direct anti-tumour activity in breast cancer. Br. J. Cancer 2010, 102, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Bosch-Barrera, J.; Merajver, S.D.; Menendez, J.A.; Van Poznak, C. Direct antitumour activity of zoledronic acid: Preclinical and clinical data. Clin. Transl. Oncol. 2011, 13, 148–155. [Google Scholar] [CrossRef]
- Senaratne, S.G.; Colston, K.W. Direct effects of bisphosphonates on breast cancer cells. Breast Cancer Res. 2002, 4, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Dumon, J.C.; Journe, F.; Kheddoumi, N.; Lagneaux, L.; Body, J.J. Cytostatic and apoptotic effects of bisphosphonates on prostate cancer cells. Eur. Urol. 2004, 45, 521–528, discussion 528–529. [Google Scholar] [CrossRef]
- Sawada, K.; Morishige, K.; Tahara, M.; Kawagishi, R.; Ikebuchi, Y.; Tasaka, K.; Murata, Y. Alendronate inhibits lysophosphatidic acid-induced migration of human ovarian cancer cells by attenuating the activation of rho. Cancer Res. 2002, 62, 6015–6020. [Google Scholar]
- Hirata, J.; Kikuchi, Y.; Kudoh, K.; Kita, T.; Seto, H. Inhibitory effects of bisphosphonates on the proliferation of human ovarian cancer cell lines and the mechanism. Med. Chem. 2006, 2, 223–226. [Google Scholar] [PubMed]
- Nagasawa, Y.; Chen, J.; Hashimoto, K. Antiarrhythmic properties of a prior oral loading of amiodarone in in vivo canine coronary ligation/reperfusion-induced arrhythmia model: Comparison with other class iii antiarrhythmic drugs. J. Pharmacol. Sci. 2005, 97, 393–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knight, L.A.; Kurbacher, C.M.; Glaysher, S.; Fernando, A.; Reichelt, R.; Dexel, S.; Reinhold, U.; Cree, I.A. Activity of mevalonate pathway inhibitors against breast and ovarian cancers in the atp-based tumour chemosensitivity assay. BMC Cancer 2009, 9, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karabulut, B.; Karaca, B.; Varol, U.; Muslu, U.; Cakar, B.; Atmaca, H.; Kisim, A.; Uzunoglu, S.; Uslu, R. Enhancing cytotoxic and apoptotic effect in ovcar-3 and mdah-2774 cells with all-trans retinoic acid and zoledronic acid: A paradigm of synergistic molecular targeting treatment for ovarian cancer. J. Exp. Clin. Cancer Res. 2010, 29, 102. [Google Scholar] [CrossRef] [Green Version]
- Atmaca, H.; Gorumlu, G.; Karaca, B.; Degirmenci, M.; Tunali, D.; Cirak, Y.; Purcu, D.U.; Uzunoglu, S.; Karabulut, B.; Sanli, U.A.; et al. Combined gossypol and zoledronic acid treatment results in synergistic induction of cell death and regulates angiogenic molecules in ovarian cancer cells. Eur. Cytokine Netw. 2009, 20, 121–130. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Kashima, H.; Rahmanto, Y.S.; Banno, K.; Yu, Y.; Matoba, Y.; Watanabe, K.; Iijima, M.; Takeda, T.; Kunitomi, H.; et al. Drug repositioning of mevalonate pathway inhibitors as antitumor agents for ovarian cancer. Oncotarget 2017, 8, 72147–72156. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, K.; Morishige, K.; Sawada, K.; Tahara, M.; Kawagishi, R.; Ikebuchi, Y.; Sakata, M.; Tasaka, K.; Murata, Y. Alendronate inhibits intraperitoneal dissemination in in vivo ovarian cancer model. Cancer Res. 2005, 65, 540–545. [Google Scholar]
- Ou, Y.J.; Chiu, H.F.; Wong, Y.H.; Yang, C.C.; Yang, Y.H. Bisphosphonate use and the risk of breast cancer: A meta-analysis of observational studies. Pharmacoepidemiol. Drug Saf. 2017, 26, 1286–1295. [Google Scholar] [CrossRef]
- Ou, Y.J.; Chiu, H.F.; Wong, Y.H.; Yang, Y.H. Bisphosphonate use and the risk of endometrial cancer: A meta-analysis of observational studies. Pharmacoepidemiol. Drug Saf. 2016, 25, 1107–1115. [Google Scholar] [CrossRef]
- Rennert, G.; Rennert, H.S.; Pinchev, M.; Lavie, O. The effect of bisphosphonates on the risk of endometrial and ovarian malignancies. Gynecol. Oncol. 2014, 133, 309–313. [Google Scholar] [CrossRef]
- Gonzalez Canga, A.; Sahagun Prieto, A.M.; Jose Diez Liebana, M.; Martinez, N.F.; Vega, M.S.; Vieitez, J.J. The pharmacokinetics and metabolism of ivermectin in domestic animal species. Vet. J. 2009, 179, 25–37. [Google Scholar] [CrossRef] [PubMed]
- McCavera, S.; Rogers, A.T.; Yates, D.M.; Woods, D.J.; Wolstenholme, A.J. An ivermectin-sensitive glutamate-gated chloride channel from the parasitic nematode haemonchus contortus. Mol. Pharmacol. 2009, 75, 1347–1355. [Google Scholar] [CrossRef] [Green Version]
- Moreno, Y.; Nabhan, J.F.; Solomon, J.; Mackenzie, C.D.; Geary, T.G. Ivermectin disrupts the function of the excretory-secretory apparatus in microfilariae of brugia malayi. Proc. Natl. Acad. Sci. USA 2010, 107, 20120–20125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, W.C. History of avermectin and ivermectin, with notes on the history of other macrocyclic lactone antiparasitic agents. Curr. Pharm. Biotechnol. 2012, 13, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Markowska, A.; Kaysiewicz, J.; Markowska, J.; Huczynski, A. Doxycycline, salinomycin, monensin and ivermectin repositioned as cancer drugs. Bioorg. Med. Chem. Lett. 2019, 29, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Drinyaev, V.A.; Mosin, V.A.; Kruglyak, E.B.; Novik, T.S.; Sterlina, T.S.; Ermakova, N.V.; Kublik, L.N.; Levitman, M.; Shaposhnikova, V.V.; Korystov, Y.N. Antitumor effect of avermectins. Eur. J. Pharmacol. 2004, 501, 19–23. [Google Scholar] [CrossRef]
- Hashimoto, H.; Messerli, S.M.; Sudo, T.; Maruta, H. Ivermectin inactivates the kinase pak1 and blocks the pak1-dependent growth of human ovarian cancer and nf2 tumor cell lines. Drug Discov. Ther. 2009, 3, 243–246. [Google Scholar]
- Melotti, A.; Mas, C.; Kuciak, M.; Lorente-Trigos, A.; Borges, I.; Ruiz i Altaba, A. The river blindness drug ivermectin and related macrocyclic lactones inhibit wnt-tcf pathway responses in human cancer. EMBO Mol. Med. 2014, 6, 1263–1278. [Google Scholar] [CrossRef]
- Sharmeen, S.; Skrtic, M.; Sukhai, M.A.; Hurren, R.; Gronda, M.; Wang, X.; Fonseca, S.B.; Sun, H.; Wood, T.E.; Ward, R.; et al. The antiparasitic agent ivermectin induces chloride-dependent membrane hyperpolarization and cell death in leukemia cells. Blood 2010, 116, 3593–3603. [Google Scholar] [CrossRef] [Green Version]
- Dominguez-Gomez, G.; Chavez-Blanco, A.; Medina-Franco, J.L.; Saldivar-Gonzalez, F.; Flores-Torrontegui, Y.; Juarez, M.; Diaz-Chavez, J.; Gonzalez-Fierro, A.; Duenas-Gonzalez, A. Ivermectin as an inhibitor of cancer stemlike cells. Mol. Med. Rep. 2018, 17, 3397–3403. [Google Scholar]
- Didier, A.; Loor, F. The abamectin derivative ivermectin is a potent p-glycoprotein inhibitor. Anticancer Drugs 1996, 7, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Dou, Q.; Chen, H.N.; Wang, K.; Yuan, K.; Lei, Y.; Li, K.; Lan, J.; Chen, Y.; Huang, Z.; Xie, N.; et al. Ivermectin induces cytostatic autophagy by blocking the pak1/akt axis in breast cancer. Cancer Res. 2016, 76, 4457–4469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juarez, M.; Schcolnik-Cabrera, A.; Duenas-Gonzalez, A. The multitargeted drug ivermectin: From an antiparasitic agent to a repositioned cancer drug. Am. J. Cancer Res. 2018, 8, 317–331. [Google Scholar]
- Liu, J.; Liang, H.; Chen, C.; Wang, X.; Qu, F.; Wang, H.; Yang, K.; Wang, Q.; Zhao, N.; Meng, J.; et al. Ivermectin induces autophagy-mediated cell death through the akt/mtor signaling pathway in glioma cells. Biosci. Rep. 2019, 39. [Google Scholar] [CrossRef]
- Liu, Y.; Fang, S.; Sun, Q.; Liu, B. Anthelmintic drug ivermectin inhibits angiogenesis, growth and survival of glioblastoma through inducing mitochondrial dysfunction and oxidative stress. Biochem. Biophys. Res. Commun. 2016, 480, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Seth, C.; Mas, C.; Conod, A.; Mueller, J.; Siems, K.; Kuciak, M.; Borges, I.; Ruiz, I.A.A. Long-lasting wnt-tcf response blocking and epigenetic modifying activities of withanolide f in human cancer cells. PLoS ONE 2016, 11, e0168170. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Gao, W.; Dou, Q.; Chen, H.; Li, Q.; Nice, E.C.; Huang, C. Ivermectin induces pak1-mediated cytostatic autophagy in breast cancer. Autophagy 2016, 12, 2498–2499. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Leibovitch, B.A.; Zeng, L.; Mezei, M.; Christova, R.; Yang, S.; Sharma, R.; Aritzia, E.; Bansal, N.; Zhou, M.M.; et al. Selamectin and ivermectin are small molecule inhibitors that interfere with sin3a-pah2 function and exert anti-tumor activity in triple-negative breast cancer. In Proceedings of the 105th Annual Meeting of the American Association for Cancer Research, Atlanta, GA USA, 5–9 April 2014; Volume 74 (Suppl. S19). [Google Scholar]
- Zhu, M.; Li, Y.; Zhou, Z. Antibiotic ivermectin preferentially targets renal cancer through inducing mitochondrial dysfunction and oxidative damage. Biochem. Biophys. Res. Commun. 2017, 492, 373–378. [Google Scholar] [CrossRef]
- Nishio, M.; Sugimachi, K.; Goto, H.; Wang, J.; Morikawa, T.; Miyachi, Y.; Takano, Y.; Hikasa, H.; Itoh, T.; Suzuki, S.O.; et al. Dysregulated yap1/taz and tgf-beta signaling mediate hepatocarcinogenesis in mob1a/1b-deficient mice. Proc. Natl. Acad. Sci. USA 2016, 113, E71–E80. [Google Scholar] [CrossRef] [Green Version]
- Kang, W.; Tong, J.H.; Chan, A.W.; Lee, T.L.; Lung, R.W.; Leung, P.P.; So, K.K.; Wu, K.; Fan, D.; Yu, J.; et al. Yes-associated protein 1 exhibits oncogenic property in gastric cancer and its nuclear accumulation associates with poor prognosis. Clin. Cancer Res. 2011, 17, 2130–2139. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.H.; Kim, Y.K.; Shin, D.H.; Lee, H.J.; Shin, N.; Kim, A.; Lee, J.H.; Choi, K.U.; Kim, J.Y.; Lee, C.H.; et al. Yes associated protein is a poor prognostic factor in well-differentiated lung adenocarcinoma. Int. J. Clin. Exp. Pathol. 2015, 8, 15933–15939. [Google Scholar] [PubMed]
- Lee, K.W.; Lee, S.S.; Kim, S.B.; Sohn, B.H.; Lee, H.S.; Jang, H.J.; Park, Y.Y.; Kopetz, S.; Kim, S.S.; Oh, S.C.; et al. Significant association of oncogene yap1 with poor prognosis and cetuximab resistance in colorectal cancer patients. Clin. Cancer Res. 2015, 21, 357–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, D.; Li, X.; He, Y.; Li, W.; Wang, Y.; Wang, H.; Jiang, S.; Xin, Y. Yap1 enhances cell proliferation, migration, and invasion of gastric cancer in vitro and in vivo. Oncotarget 2016, 7, 81062–81076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, Y.; Chang, T.; Wang, Y.; Liu, Y.; Li, W.; Li, M.; Fan, H.Y. Yap promotes ovarian cancer cell tumorigenesis and is indicative of a poor prognosis for ovarian cancer patients. PLoS ONE 2014, 9, e91770. [Google Scholar] [CrossRef] [PubMed]
- Nambara, S.; Masuda, T.; Nishio, M.; Kuramitsu, S.; Tobo, T.; Ogawa, Y.; Hu, Q.; Iguchi, T.; Kuroda, Y.; Ito, S.; et al. Antitumor effects of the antiparasitic agent ivermectin via inhibition of yes-associated protein 1 expression in gastric cancer. Oncotarget 2017, 8, 107666–107677. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xu, Y.; Wan, H.; Hu, J. Antibiotic ivermectin selectively induces apoptosis in chronic myeloid leukemia through inducing mitochondrial dysfunction and oxidative stress. Biochem. Biophys. Res. Commun. 2018, 497, 241–247. [Google Scholar] [CrossRef]
- Kodama, M.; Kodama, T.; Newberg, J.Y.; Katayama, H.; Kobayashi, M.; Hanash, S.M.; Yoshihara, K.; Wei, Z.; Tien, J.C.; Rangel, R.; et al. In vivo loss-of-function screens identify kpnb1 as a new druggable oncogene in epithelial ovarian cancer. Proc. Natl. Acad. Sci. USA 2017, 114, E7301–E7310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Qin, T.; Zhu, Z.; Hong, F.; Xu, Y.; Zhang, X.; Xu, X.; Ma, A. Ivermectin augments the in vitro and in vivo efficacy of cisplatin in epithelial ovarian cancer by suppressing akt/mtor signaling. Am. J. Med. Sci. 2020, 359, 123–129. [Google Scholar] [CrossRef]
- Jiang, L.; Wang, P.; Sun, Y.J.; Wu, Y.J. Ivermectin reverses the drug resistance in cancer cells through egfr/erk/akt/nf-kappab pathway. J. Exp. Clin. Cancer Res. 2019, 38, 265. [Google Scholar] [CrossRef]
- Lestner, J.; Hope, W.W. Itraconazole: An update on pharmacology and clinical use for treatment of invasive and allergic fungal infections. Expert Opin. Drug Metab. Toxicol. 2013, 9, 911–926. [Google Scholar] [CrossRef]
- Pandya, N.A.; Atra, A.A.; Riley, U.; Pinkerton, C.R. Role of itraconazole in haematology/oncology. Arch. Dis. Child. 2003, 88, 258–260. [Google Scholar] [CrossRef] [PubMed]
- Pounds, R.; Leonard, S.; Dawson, C.; Kehoe, S. Repurposing itraconazole for the treatment of cancer. Oncol. Lett. 2017, 14, 2587–2597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, J.S.; Liu, J.O. Recent advances in drug repositioning for the discovery of new anticancer drugs. Int. J. Biol. Sci. 2014, 10, 654–663. [Google Scholar] [CrossRef] [Green Version]
- Pantziarka, P.; Sukhatme, V.; Bouche, G.; Meheus, L.; Sukhatme, V.P. Repurposing drugs in oncology (redo)-itraconazole as an anti-cancer agent. Ecancermedicalscience 2015, 9, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Aftab, B.T.; Tang, J.Y.; Kim, D.; Lee, A.H.; Rezaee, M.; Kim, J.; Chen, B.; King, E.M.; Borodovsky, A.; et al. Itraconazole and arsenic trioxide inhibit hedgehog pathway activation and tumor growth associated with acquired resistance to smoothened antagonists. Cancer Cell 2013, 23, 23–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Tang, J.Y.; Gong, R.; Kim, J.; Lee, J.J.; Clemons, K.V.; Chong, C.R.; Chang, K.S.; Fereshteh, M.; Gardner, D.; et al. Itraconazole, a commonly used antifungal that inhibits hedgehog pathway activity and cancer growth. Cancer Cell 2010, 17, 388–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.; Li, J.; Zhang, T.; Zou, L.; Chen, Y.; Wang, K.; Lei, Y.; Yuan, K.; Li, Y.; Lan, J.; et al. Itraconazole suppresses the growth of glioblastoma through induction of autophagy: Involvement of abnormal cholesterol trafficking. Autophagy 2014, 10, 1241–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Head, S.A.; Shi, W.Q.; Yang, E.J.; Nacev, B.A.; Hong, S.Y.; Pasunooti, K.K.; Li, R.J.; Shim, J.S.; Liu, J.O. Simultaneous targeting of npc1 and vdac1 by itraconazole leads to synergistic inhibition of mtor signaling and angiogenesis. ACS Chem. Biol. 2017, 12, 174–182. [Google Scholar] [CrossRef]
- Hu, Q.; Hou, Y.C.; Huang, J.; Fang, J.Y.; Xiong, H. Itraconazole induces apoptosis and cell cycle arrest via inhibiting hedgehog signaling in gastric cancer cells. J. Exp. Clin. Cancer Res. 2017, 36, 50. [Google Scholar] [CrossRef] [Green Version]
- Liang, G.; Liu, M.; Wang, Q.; Shen, Y.; Mei, H.; Li, D.; Liu, W. Itraconazole exerts its anti-melanoma effect by suppressing hedgehog, wnt, and pi3k/mtor signaling pathways. Oncotarget 2017, 8, 28510–28525. [Google Scholar] [CrossRef] [Green Version]
- Tsubamoto, H.; Inoue, K.; Sakata, K.; Ueda, T.; Takeyama, R.; Shibahara, H.; Sonoda, T. Itraconazole inhibits akt/mtor signaling and proliferation in endometrial cancer cells. Anticancer Res. 2017, 37, 515–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, T.; Tsubamoto, H.; Inoue, K.; Sakata, K.; Shibahara, H.; Sonoda, T. Itraconazole modulates hedgehog, wnt/beta-catenin, as well as akt signalling, and inhibits proliferation of cervical cancer cells. Anticancer Res. 2017, 37, 3521–3526. [Google Scholar] [PubMed] [Green Version]
- Chong, C.R.; Xu, J.; Lu, J.; Bhat, S.; Sullivan, D.J., Jr.; Liu, J.O. Inhibition of angiogenesis by the antifungal drug itraconazole. ACS Chem. Biol. 2007, 2, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Ban, L.; Mei, T.; Su, Q.; Li, W.; Huang, Z.; Liu, L.; Wu, Y.; Lv, S.; Wang, A.; Li, S. Anti-fungal drug itraconazole exerts anti-cancer effects in oral squamous cell carcinoma via suppressing hedgehog pathway. Life Sci. 2020, 254, 117695. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Cheng, L.; Qian, W.; Jiang, Z.; Sun, L.; Zhao, Y.; Zhou, Y.; Zhao, L.; Wang, P.; Duan, W.; et al. Itraconazole inhibits invasion and migration of pancreatic cancer cells by suppressing tgf-beta/smad2/3 signaling. Oncol. Rep. 2018, 39, 1573–1582. [Google Scholar]
- Chen, M.B.; Liu, Y.Y.; Xing, Z.Y.; Zhang, Z.Q.; Jiang, Q.; Lu, P.H.; Cao, C. Itraconazole-induced inhibition on human esophageal cancer cell growth requires ampk activation. Mol. Cancer Ther. 2018, 17, 1229–1239. [Google Scholar] [CrossRef] [Green Version]
- Lan, K.; Yan, R.; Zhu, K.; Li, W.; Xu, Z.; Dang, C.; Li, K. Itraconazole inhibits the proliferation of gastric cancer cells in vitro and improves patient survival. Oncol. Lett. 2018, 16, 3651–3657. [Google Scholar] [CrossRef] [Green Version]
- Choi, C.H.; Ryu, J.Y.; Cho, Y.J.; Jeon, H.K.; Choi, J.J.; Ylaya, K.; Lee, Y.Y.; Kim, T.J.; Chung, J.Y.; Hewitt, S.M.; et al. The anti-cancer effects of itraconazole in epithelial ovarian cancer. Sci. Rep. 2017, 7, 6552. [Google Scholar] [CrossRef] [Green Version]
- Ally, M.S.; Ransohoff, K.; Sarin, K.; Atwood, S.X.; Rezaee, M.; Bailey-Healy, I.; Kim, J.; Beachy, P.A.; Chang, A.L.; Oro, A.; et al. Effects of combined treatment with arsenic trioxide and itraconazole in patients with refractory metastatic basal cell carcinoma. JAMA Dermatol. 2016, 152, 452–456. [Google Scholar] [CrossRef]
- Tsubamoto, H.; Sonoda, T.; Ikuta, S.; Tani, S.; Inoue, K.; Yamanaka, N. Combination chemotherapy with itraconazole for treating metastatic pancreatic cancer in the second-line or additional setting. Anticancer Res. 2015, 35, 4191–4196. [Google Scholar]
- Tsubamoto, H.; Sonoda, T.; Yamasaki, M.; Inoue, K. Impact of combination chemotherapy with itraconazole on survival of patients with refractory ovarian cancer. Anticancer Res. 2014, 34, 2481–2487. [Google Scholar]
- Correia, A.; Silva, D.; Correia, A.; Vilanova, M.; Gartner, F.; Vale, N. Study of new therapeutic strategies to combat breast cancer using drug combinations. Biomolecules 2018, 8, 175. [Google Scholar] [CrossRef] [Green Version]
- Hara, M.; Nagasaki, T.; Shiga, K.; Takeyama, H. Suppression of cancer-associated fibroblasts and endothelial cells by itraconazole in bevacizumab-resistant gastrointestinal cancer. Anticancer Res. 2016, 36, 169–177. [Google Scholar]
- Antonarakis, E.S.; Heath, E.I.; Smith, D.C.; Rathkopf, D.; Blackford, A.L.; Danila, D.C.; King, S.; Frost, A.; Ajiboye, A.S.; Zhao, M.; et al. Repurposing itraconazole as a treatment for advanced prostate cancer: A noncomparative randomized phase ii trial in men with metastatic castration-resistant prostate cancer. Oncologist 2013, 18, 163–173. [Google Scholar] [CrossRef]
- Kim, D.J.; Kim, J.; Spaunhurst, K.; Montoya, J.; Khodosh, R.; Chandra, K.; Fu, T.; Gilliam, A.; Molgo, M.; Beachy, P.A.; et al. Open-label, exploratory phase ii trial of oral itraconazole for the treatment of basal cell carcinoma. J. Clin. Oncol. 2014, 32, 745–751. [Google Scholar] [CrossRef]
- Rudin, C.M.; Brahmer, J.R.; Juergens, R.A.; Hann, C.L.; Ettinger, D.S.; Sebree, R.; Smith, R.; Aftab, B.T.; Huang, P.; Liu, J.O. Phase 2 study of pemetrexed and itraconazole as second-line therapy for metastatic nonsquamous non-small-cell lung cancer. J. Thorac. Oncol. 2013, 8, 619–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsubamoto, H.; Sonoda, T.; Inoue, K. Impact of itraconazole on the survival of heavily pre-treated patients with triple-negative breast cancer. Anticancer Res. 2014, 34, 3839–3844. [Google Scholar]
- Mamtani, R.; Yang, Y.X.; Scott, F.I.; Lewis, J.D.; Boursi, B. Association of itraconazole, a hedgehog inhibitor, and bladder cancer. J. Urol. 2016, 196, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Inoue, K.; Tsubamoto, H.; Sakata, K.; Sakane, R.; Hao, H.; Hirota, S.; Sonoda, T.; Shibahara, H. Expression of hedgehog signals and growth inhibition by itraconazole in endometrial cancer. Anticancer Res. 2016, 36, 149–153. [Google Scholar]
- Tsubamoto, H.; Sonoda, T.; Ikuta, S.; Tani, S.; Inoue, K.; Yamanaka, N. Impact of itraconazole after first-line chemotherapy on survival of patients with metastatic biliary tract cancer. Anticancer Res. 2015, 35, 4923–4927. [Google Scholar] [CrossRef] [PubMed]
- Vreugdenhil, G.; Raemaekers, J.M.; van Dijke, B.J.; de Pauw, B.E. Itraconazole and multidrug resistance: Possible effects on remission rate and disease-free survival in acute leukemia. Ann. Hematol. 1993, 67, 107–109. [Google Scholar] [CrossRef]
- Shirakawa, K.; Takara, K.; Tanigawara, Y.; Aoyama, N.; Kasuga, M.; Komada, F.; Sakaeda, T.; Okumura, K. Interaction of docetaxel (“taxotere”) with human p-glycoprotein. Jpn. J. Cancer Res. 1999, 90, 1380–1386. [Google Scholar] [CrossRef]
- Takara, K.; Tanigawara, Y.; Komada, F.; Nishiguchi, K.; Sakaeda, T.; Okumura, K. Cellular pharmacokinetic aspects of reversal effect of itraconazole on p-glycoprotein-mediated resistance of anticancer drugs. Biol. Pharm. Bull. 1999, 22, 1355–1359. [Google Scholar] [CrossRef] [Green Version]
- Oldfield, V.; Plosker, G.L. Lopinavir/ritonavir: A review of its use in the management of hiv infection. Drugs 2006, 66, 1275–1299. [Google Scholar] [CrossRef]
- Kumar, S.; Bryant, C.S.; Chamala, S.; Qazi, A.; Seward, S.; Pal, J.; Steffes, C.P.; Weaver, D.W.; Morris, R.; Malone, J.M.; et al. Ritonavir blocks akt signaling, activates apoptosis and inhibits migration and invasion in ovarian cancer cells. Mol. Cancer 2009, 8, 26. [Google Scholar] [CrossRef] [Green Version]
- Carroll, V.; Garzino-Demo, A. Hiv-associated lymphoma in the era of combination antiretroviral therapy: Shifting the immunological landscape. Pathog. Dis. 2015, 73, ftv044. [Google Scholar] [CrossRef]
- Shmakova, A.; Germini, D.; Vassetzky, Y. Hiv-1, haart and cancer: A complex relationship. Int. J. Cancer 2020, 146, 2666–2679. [Google Scholar] [CrossRef]
- Cheung, T.W. Aids-related cancer in the era of highly active antiretroviral therapy (haart): A model of the interplay of the immune system, virus, and cancer. “On the offensive--the trojan horse is being destroyed”--part b: Malignant lymphoma. Cancer Investig. 2004, 22, 787–798. [Google Scholar] [CrossRef]
- Laurence, J. Impact of haart on hiv-linked malignancies. AIDS Read. 2003, 13, 202–205. [Google Scholar]
- Monini, P.; Toschi, E.; Sgadari, C.; Bacigalupo, I.; Palladino, C.; Carlei, D.; Barillari, G.; Ensoli, B. The use of haart for biological tumour therapy. J. HIV Ther. 2006, 11, 53–56. [Google Scholar]
- Ntekim, A.; Campbell, O.; Rothenbacher, D. Optimal management of cervical cancer in hiv-positive patients: A systematic review. Cancer Med. 2015, 4, 1381–1393. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Polesel, J.; Rickenbach, M.; Dal Maso, L.; Keiser, O.; Kofler, A.; Rapiti, E.; Levi, F.; Jundt, G.; Fisch, T.; et al. Cancer risk in the swiss hiv cohort study: Associations with immunodeficiency, smoking, and highly active antiretroviral therapy. J. Natl. Cancer Inst. 2005, 97, 425–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kincaid, L. Modern haart decreases cancers in children with hiv. Lancet Oncol. 2007, 8, 103. [Google Scholar] [CrossRef]
- Long, J.L.; Engels, E.A.; Moore, R.D.; Gebo, K.A. Incidence and outcomes of malignancy in the haart era in an urban cohort of hiv-infected individuals. AIDS 2008, 22, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Franzetti, M.; Ricci, E.; Bonfanti, P. The pattern of non-aids-defining cancers in the hiv population: Epidemiology, risk factors and prognosis. A review. Curr. HIV Res. 2019, 17, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Dewan, M.Z.; Uchihara, J.N.; Terashima, K.; Honda, M.; Sata, T.; Ito, M.; Fujii, N.; Uozumi, K.; Tsukasaki, K.; Tomonaga, M.; et al. Efficient intervention of growth and infiltration of primary adult t-cell leukemia cells by an hiv protease inhibitor, ritonavir. Blood 2006, 107, 716–724. [Google Scholar] [CrossRef] [Green Version]
- Ikezoe, T.; Daar, E.S.; Hisatake, J.; Taguchi, H.; Koeffler, H.P. Hiv-1 protease inhibitors decrease proliferation and induce differentiation of human myelocytic leukemia cells. Blood 2000, 96, 3553–3559. [Google Scholar] [CrossRef]
- Labo, N.; Miley, W.; Benson, C.A.; Campbell, T.B.; Whitby, D. Epidemiology of kaposi’s sarcoma-associated herpesvirus in hiv-1-infected us persons in the era of combination antiretroviral therapy. AIDS 2015, 29, 1217–1225. [Google Scholar] [CrossRef]
- Noy, A. Optimizing treatment of hiv-associated lymphoma. Blood 2019, 134, 1385–1394. [Google Scholar] [CrossRef]
- Mazzocchi, A.R.; Rajan, S.A.P.; Votanopoulos, K.I.; Hall, A.R.; Skardal, A. In vitro patient-derived 3d mesothelioma tumor organoids facilitate patient-centric therapeutic screening. Sci. Rep. 2018, 8, 2886. [Google Scholar] [CrossRef] [Green Version]
- Meijer, T.G.; Naipal, K.A.; Jager, A.; van Gent, D.C. Ex vivo tumor culture systems for functional drug testing and therapy response prediction. Future Sci. OA 2017, 3, FSO190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ince, T.A.; Sousa, A.D.; Jones, M.A.; Harrell, J.C.; Agoston, E.S.; Krohn, M.; Selfors, L.M.; Liu, W.; Chen, K.; Yong, M.; et al. Characterization of twenty-five ovarian tumour cell lines that phenocopy primary tumours. Nat. Commun. 2015, 6, 7419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swords, R.T.; Azzam, D.; Al-Ali, H.; Lohse, I.; Volmar, C.H.; Watts, J.M.; Perez, A.; Rodriguez, A.; Vargas, F.; Elias, R.; et al. Ex-vivo sensitivity profiling to guide clinical decision making in acute myeloid leukemia: A pilot study. Leuk. Res. 2018, 64, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Ghani, F.I.; Dendo, K.; Watanabe, R.; Yamada, K.; Yoshimatsu, Y.; Yugawa, T.; Nakahara, T.; Tanaka, K.; Yoshida, H.; Yoshida, M.; et al. An ex-vivo culture system of ovarian cancer faithfully recapitulating the pathological features of primary tumors. Cells 2019, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, L.; Tighe, A.; Golder, A.; Littler, S.; Bakker, B.; Moralli, D.; Murtuza Baker, S.; Donaldson, I.J.; Spierings, D.C.J.; Wardenaar, R.; et al. A living biobank of ovarian cancer ex vivo models reveals profound mitotic heterogeneity. Nat. Commun. 2020, 11, 822. [Google Scholar] [CrossRef] [PubMed]
- Lohse, I.; Al-Ali, H.; Volmar, C.H.; A, D.A.T.; Brothers, S.P.; Capobianco, A.J.; Wahlestedt, C. Ex vivo drug sensitivity testing as a means for drug repurposing in esophageal adenocarcinoma. PLoS ONE 2018, 13, e0203173. [Google Scholar] [CrossRef]
- Murumägi, A.; Ungureanu, D.; Khan, S.; Hirasawa, A.; Arjama, M.; Välimäki, K.; Mikkonen, P.; Niininen, W.; Kumar, A.; Eldfors, S.; et al. Clinical implementation of precision systems oncology in the treatment of ovarian cancer based on ex-vivo drug testing and molecular profiling. In Proceedings of the Annual Meeting of the American Association for Cancer Research: Experimental and Molecular Therapeutics, Atlanta, GA, USA, 29 March–3 April 2019; Volume 79, p. 2945. [Google Scholar]
- Lohmussaar, K.; Boretto, M.; Clevers, H. Human-derived model systems in gynecological cancer research. Trends Cancer 2020. [Google Scholar] [CrossRef]
- Lengyel, E. Ovarian cancer development and metastasis. Am. J. Pathol. 2010, 177, 1053–1064. [Google Scholar] [CrossRef]
- Ahmed, N.; Stenvers, K.L. Getting to know ovarian cancer ascites: Opportunities for targeted therapy-based translational research. Front. Oncol. 2013, 3, 256. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, N.; Riley, C.; Oliva, K.; Rice, G.; Quinn, M. Ascites induces modulation of alpha6beta1 integrin and urokinase plasminogen activator receptor expression and associated functions in ovarian carcinoma. Br. J. Cancer 2005, 92, 1475–1485. [Google Scholar] [CrossRef] [Green Version]
- Vlachogiannis, G.; Hedayat, S.; Vatsiou, A.; Jamin, Y.; Fernandez-Mateos, J.; Khan, K.; Lampis, A.; Eason, K.; Huntingford, I.; Burke, R.; et al. Patient-derived organoids model treatment response of metastatic gastrointestinal cancers. Science 2018, 359, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Weeber, F.; Ooft, S.N.; Dijkstra, K.K.; Voest, E.E. Tumor organoids as a pre-clinical cancer model for drug discovery. Cell Chem. Biol. 2017, 24, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A.; Plummer, E.R.; Elattar, A.; Soohoo, S.; Uzir, B.; Quinn, J.E.; McCluggage, W.G.; Maxwell, P.; Aneke, H.; Curtin, N.J.; et al. Clinicopathological features of homologous recombination-deficient epithelial ovarian cancers: Sensitivity to parp inhibitors, platinum, and survival. Cancer Res. 2012, 72, 5675–5682. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.; Sanderson, P.E.; Zheng, W. Drug combination therapy increases successful drug repositioning. Drug Discov. Today 2016, 21, 1189–1195. [Google Scholar] [CrossRef]
Figure 1. Mechanism of action of non-oncological drugs in ovarian cancer (OC). Statins inhibit 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR) leading to the blocking of cholesterol biosynthetic pathway though a mevalonate-dependent mechanism. Moreover, statins can block drug efflux pumps by a mevalonate-independent mechanism. Bisphosphonates block farnesyl pyrophosphate synthase, located downstream HMGCR, leading to the impairment of cholesterol biosynthesis. Metformin inhibits insulin signals and glucose synthesis via respiratory-chain complex I blockage. Ritonavir is a protease inhibitor that inhibits the production of phosphorylated protein kinase B (AKT) leading to the impairment of phosphatidylinositol 3-kinases (PI3K)-Akt pathway. Itraconazole can inhibit Hedgehog, mammalian target of rapamycin (mTOR), and Wnt signalling pathway. Moreover, itraconazole can inhibit angiogenesis and lymphangiogenesis, and promote the overexpression of P-glycoprotein. Ivermectin interferes with several cellular mechanisms, including multidrug resistance proteins (MDR) inhibition, Akt/mTOR, and Wnt signalling pathways modulation, p21–activated kinase (PAK-1) and yes-associated protein 1 (YAP1). Moreover, ivermectin promotes the increase of intracellular reactive oxygen species (ROS) levels leading to the downregulation of stemness genes. Adenosine diphosphate (ADP); adenosine monophosphate (AMP); adenosine triphosphate (ATP); 3-Hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA).
Figure 1. Mechanism of action of non-oncological drugs in ovarian cancer (OC). Statins inhibit 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR) leading to the blocking of cholesterol biosynthetic pathway though a mevalonate-dependent mechanism. Moreover, statins can block drug efflux pumps by a mevalonate-independent mechanism. Bisphosphonates block farnesyl pyrophosphate synthase, located downstream HMGCR, leading to the impairment of cholesterol biosynthesis. Metformin inhibits insulin signals and glucose synthesis via respiratory-chain complex I blockage. Ritonavir is a protease inhibitor that inhibits the production of phosphorylated protein kinase B (AKT) leading to the impairment of phosphatidylinositol 3-kinases (PI3K)-Akt pathway. Itraconazole can inhibit Hedgehog, mammalian target of rapamycin (mTOR), and Wnt signalling pathway. Moreover, itraconazole can inhibit angiogenesis and lymphangiogenesis, and promote the overexpression of P-glycoprotein. Ivermectin interferes with several cellular mechanisms, including multidrug resistance proteins (MDR) inhibition, Akt/mTOR, and Wnt signalling pathways modulation, p21–activated kinase (PAK-1) and yes-associated protein 1 (YAP1). Moreover, ivermectin promotes the increase of intracellular reactive oxygen species (ROS) levels leading to the downregulation of stemness genes. Adenosine diphosphate (ADP); adenosine monophosphate (AMP); adenosine triphosphate (ATP); 3-Hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA).

Figure 2. Establishment of ex vivo models from ascitic fluid-derived cancer cells to perform drug efficacy tests. Combination of drug repurposing (e.g., pitavastatin, metformin, bisphosphonates, ivermectin, itraconazole and ritonavir) with conventional chemotherapy (e.g., carboplatin and paclitaxel) may have the benefits of increased efficacy and has potential to decrease the risk of therapeutic failure. The effectiveness of drug repurposing approaches to target or sensitize chemoresistant cells to conventional chemotherapy can be validate in established ex vivo models. A schematic diagram demonstrating the conventional chemotherapy in combination with compounds of drug repurposing that can directly target the chemoresistant cell and tumour loses its ability to generate new cancer cells, or sensitize chemoresistant cells in order to disrupt the stemness and make them more sensitive to conventional chemotherapy.
Figure 2. Establishment of ex vivo models from ascitic fluid-derived cancer cells to perform drug efficacy tests. Combination of drug repurposing (e.g., pitavastatin, metformin, bisphosphonates, ivermectin, itraconazole and ritonavir) with conventional chemotherapy (e.g., carboplatin and paclitaxel) may have the benefits of increased efficacy and has potential to decrease the risk of therapeutic failure. The effectiveness of drug repurposing approaches to target or sensitize chemoresistant cells to conventional chemotherapy can be validate in established ex vivo models. A schematic diagram demonstrating the conventional chemotherapy in combination with compounds of drug repurposing that can directly target the chemoresistant cell and tumour loses its ability to generate new cancer cells, or sensitize chemoresistant cells in order to disrupt the stemness and make them more sensitive to conventional chemotherapy.

|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nunes, M.; Henriques Abreu, M.; Bartosch, C.; Ricardo, S. Recycling the Purpose of Old Drugs to Treat Ovarian Cancer. Int. J. Mol. Sci. 2020, 21, 7768. https://doi.org/10.3390/ijms21207768
AMA Style
Nunes M, Henriques Abreu M, Bartosch C, Ricardo S. Recycling the Purpose of Old Drugs to Treat Ovarian Cancer. International Journal of Molecular Sciences. 2020; 21(20):7768. https://doi.org/10.3390/ijms21207768
Chicago/Turabian StyleNunes, Mariana, Miguel Henriques Abreu, Carla Bartosch, and Sara Ricardo. 2020. "Recycling the Purpose of Old Drugs to Treat Ovarian Cancer" International Journal of Molecular Sciences 21, no. 20: 7768. https://doi.org/10.3390/ijms21207768
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.