
On the order of 90,000 US deaths in 2021 and uncountable hospitalizations could be prevented by delaying dose 2 timing similar to what the UK, Canada, and Denmark are doing.
Make that 70,000 because we lost January.
Make that 45,000 because we lost February.
Make that 25,000 because we lost March. Will we lose April? -ugh
note: any debate about the exact 10K’s of lives at stake has missed the point.
and, more of the world may follow the UK, Canada, Denmark, Germany and US, saving even more lives.
It is proposed that the benefits of deferring dose 2 outweigh the risks.
Is there any plan that would achieve better results?
Reduced:
- morbidity
- hospitalizations
- transmission
- total replication/mutation
- dose 2 side-effects
- world-wide shortage of vaccine
To date, there are no credible arguments of risk that haven’t been addressed herein. Contact Really Correct with your concerns and they will be addressed here within 3 days.
Fully reopen faster and with greater safety by encouraging delay of dose 2.
Evidence For COVID-19 Vaccine Deferred Dose 2 Boost Timing https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3760833

“there is no biological reason why receiving the second dose late would diminish the effectiveness of the vaccine, provided it’s received before too long an interval.” – Paul Sax, M.D., Professor of Medicine, Harvard Medical School
“if it is not feasible to adhere to the recommended interval, the second dose of Pfizer-BioNTech and Moderna COVID-19 vaccines may be scheduled for administration up to 6 weeks (42 days) after the first dose. There are currently limited data on efficacy of mRNA COVID-19 vaccines administered beyond this window. If the second dose is administered beyond these intervals, there is no need to restart the series.” – CDC 1/21/2021
 Loading…
Loading…
More Evidence
“We urge consideration of interim use of single doses in the United States in order to extend vaccination to as many people as possible. Based on immunologic principles, sensitization with single doses would still allow boosting with a second dose several months later, when supplies improve.” Oxford Academic accepted manuscript “Accelerate COVID-19 Vaccine Rollout by Delaying the Second Dose of mRNA Vaccines” by Stanley A. Plotkin, MD, Emeritus Professor of Pediatrics, University of Pennsylvania, Award for Achievement in Vaccinology and Immunology and 10 other awards , Neal Halsey, MD, Johns Hopkins University Bloomberg School of Public Health. Bloomberg School of Public Health


“Each time we elect the latter strategy, the time interval between the first shot and the booster will widen. When, then, do we change course? We could wait until we have overwhelming supply, but given the global need that won’t be any time soon. Or we could change course when the data tell us the immunity from the first shot is waning to a level where the booster is the best next use of the vaccine.” – Peter B. Bach, MD, Memorial Sloan Kettering Cancer Center – and based on tons of existing immunological infection data – that would likely be in 3-8 months, with 3-5 being better at preserving the longest level of sterilizing immunity congruent with the vaccination rollout period.

“we should give people a single vaccination now and defer their second shot until more doses of vaccine become available.” – Robert M. Wachter is chair of the department of medicine at the University of California at San Francisco. Ashish K. Jha is dean of the Brown University School of Public Health.
“Your immune system is really smart,” said Dr. Buddy Creech, director of the Vanderbilt Vaccine Research Program at Vanderbilt University Medical Center in Nashville, Tennessee. “It doesn’t forget what it saw the first time,” he said, referring to the first vaccine dose. Creech, who has overseen clinical trials for Moderna, said the vaccines should work as expected, even if the second dose is delayed a month or more than what is recommended. “Do not panic. Even if it’s four weeks, six weeks, eight weeks before you can get that second dose, it’s fine from an immune system standpoint,” he said.
“Longer intervals favor higher immune protection,” said David Salisbury, an infectious-disease expert and former director of immunization for the U.K. government.“
“U.K. regulators and government scientists said they have to make trade-offs to prevent deaths and prevent the collapse of the state-run health service. They are buying time until more vaccines become available. They also said they are basing guidance not on these vaccine trials alone but on broader science and experience. “Clearly, if we had infinite vaccine, we might have taken different approaches, but we don’t,” Chris Whitty, England’s chief medical officer, told reporters about the dosing decisions.””
This AstraZeneca data demonstrates well established generic immune response behavior to both vaccines and infections and it applies in principle to vaccines and infections as an immunologic principle: “The efficacy rate rose to 82.4% when there was at least a 12-week interval before the second dose. When the second dose was given less than six weeks after the first one, the efficacy rate was 54.9%.” This could be expected because “the 2nd dose antigens have a probability of binding to any antibody titer remaining from the dose 1 immune response, preventing the antigen from interacting with B / T cells which is necessary to improve binding affinity (immunity). An appropriate delay allows antibody response to wane from it’s peak and enables a higher probability of B / T / antigen re-activation and further SHM responses within germinal centers. Existing B / T mem, antibodies, etc. remain protective during the period between doses“.
“Our vaccine because neutralizing antibody activity is comparable to other Covid-19 vaccines that have shown activity against more serious diseases, especially when the dosing interval is optimized for 8-12 weeks. I am confident that it can protect against serious illness. “

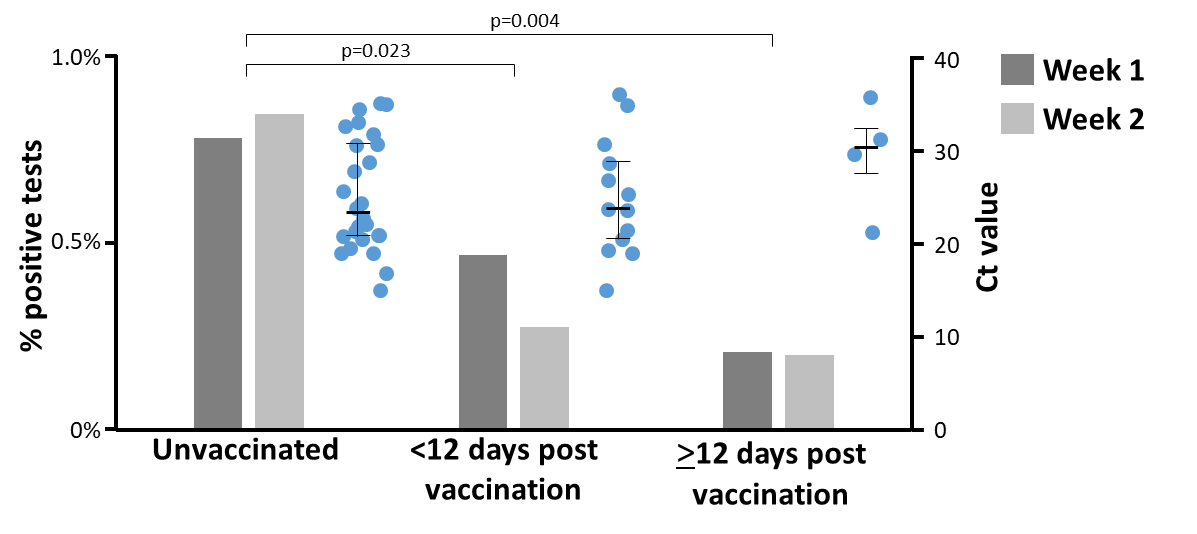
Regarding real-world data from Israel: “Estimated vaccine effectiveness was pretty much 0 at day 14 but then rose to about 90% at day 21 before levelling off. The cause of the initial surge in infection risk is unknown but may be related to people being less cautious about maintaining protective behaviours as soon as they have the injection. What our analysis shows is that a single dose of vaccine is highly protective, although it can take up to 21 days to achieve this.”
“In December, 2020, the Israeli Government approved the BNT162b2 COVID-19 vaccine and initiated a national immunisation campaign prioritising health-care workers (HCWs), as in other countries” “Adjusted rate reductions of COVID-19 disease were … 85% (71–92) for … days 15–28 after the first dose.” – Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients – The Lancet





“Also on Monday, the province announced it is extending the time between first and second doses of COVID-19 vaccine to four months. The change, as well as Health Canada’s approval of a third vaccine, means every eligible person in B.C. will receive the first dose of their vaccine by mid- to late July.”

Canada’s National Advisory Committee on Immunization (NACI) now says the maximum interval between the first and second doses of the Pfizer-BioNTech vaccine should increase from three weeks to four months.“NACI recommends that in the context of limited COVID-19 vaccine supply, jurisdictions should maximize the number of individuals benefiting from the first dose of vaccine by extending the second dose of COVID-19 vaccine up to four months after the first,” the committee said in a statement.

“‘A single dose of vaccine may be considered for individuals with previous SARS-CoV-2 infection, symptomatic or asymptomatic’, the ministry statement said. The recommendation applies to people diagnosed with COVID between three and six months previously. France and Spain announced a similar policy last month”
Note the timing of 3 to 6 months between infection (which mimics dose 1), and a dose of the vaccine (which mimics dose 2). Apparently, Italy thinks dose 2 should follow an infection no earlier than 3 months, but can be delayed as long as 6 months.

On March 5th, after losing many people, an article appears showing Germany has decided in favor of delaying dose 2 as the UK is doing.



Mutating Viral Escape
Some concern about a mutating virus escaping the vaccine has been expressed. What must be understood is that, as viral replication increases, so does potential for mutation. A 2x population vaccinated with dose 1 produces far fewer total viral replications than does a 1x population with 2 doses. Mutations are not “intelligent” such that they “scheme” on how to evade the immune system, mutations are random. And the random occurrence depends upon large amounts of viral replication. A single dose dramatically reduces that replication opportunity, whereas a 2nd dose within the first several months only marginally reduces replication. After many months, dose 2 importance increases with time. A 2x population vaccinated with dose 1 produces far fewer total viral replications than does a 1x population with 2 doses. Any selective pressure that might occur does so within a smaller unvaccinated population which reduces total replications when partial immunity (that hinders replication) exists within the vaccinated (and/or infection recovered) population. A 2x population vaccinated with dose 1 produces far fewer total viral replications than does a 1x population with 2 doses.
Whether considering the case of a new variant development, further replication of an existing variant, or developing a variant of a variant, when comparing a vaccinated individual versus an unvaccinated individual, more viral replication of the specific infective pathogen[s], and potential for further mutation of that pathogen, will occur in the unvaccinated individual, regardless of any selective pressure. It is ludicrous to suggest that a person vaccinated with only 1 dose, because of selective pressure, would somehow replicate MORE virus than the same person being unvaccinated. Increasing the vaccinated population, even if with reduced efficacy, results in fewer total replications.
Additionally, concern about viral escape often ignores the fact that the immune system, while primed by the vaccine to respond rapidly, will also respond additionally as needed to clear the virus, regardless of that initial vaccine induced immunity. And, being mutable, it will adapt to variants. The vaccine provides a dramatic lead in the exponential war between virus and immune system; and it is the immune system that continues to adapt and work to clear the virus as long as it is present. The virus stimulates B cell proliferation, plasma cell maturity, and antibody secretion. When the virus is no longer present, that stimulus diminishes and the immune system no longer continues to be stimulated. The virus is eliminated. Variants are much more likely to develop in a mostly non-immune population as has been the case for all of the variants such as B.1.117 and B.1.351 that developed prior to vaccine availability. To reduce variants, it is better to have a 2x vaccinated population even if efficacy is marginally reduced relative to that of a marginally improved vaccine efficacy in a 1x population.
Furthermore, “The protective immune responses that vaccines elicit tend to keep pathogen populations from ever achieving large sizes, reducing the accumulation of diversity and opportunities for onward transmission.”, and “The different antibody repertoires observed between subjects is due to the numerous mechanisms that generate antibody diversity during immune development [66,68]. Indeed, minimal overlap of immune repertoires is quite common [70] suggesting that vaccination also creates mosaic-like patterns in host populations. The high multiplicity of therapeutic vaccine targets thus reduces the chance that resistance will originate and the ability of resistance to spread should it originate”. Polyclonal sera developed by immune responses to real infections and vaccines that encompass the majority viral proteins / entire “spike”, create redundant overlapping mechanisms of neutralizing a variant virus. While the prior B / T / antibodies may have reduced neutralizing effect, any unbound virus will activate additional plasma cell proliferation and antibody secretion as a compensating effect which serves to limit viral replication while additional variant specific polyclones develop. The immune response adaptation to the variant will further serve to clear the virus as clones specific to the variant complete their maturation / affinity increasing processes. Minor variants tend to be rapidly cleared, while more significant variants are slowed, resulting in less viral replication, until they are cleared by a larger number of antibodies and/or more specific antibody clones that develop. Symptoms are likely to vary accordingly.
Johnson & Johnson Janssen vaccine “Demonstrated Complete Protection Against COVID-19 related Hospitalization and Death as of Day 28″ … “Protection Against Severe Disease Across Geographies, Ages, and Multiple Virus Variants, including the SARS-CoV-2 Variant from the B.1.351 Lineage Observed in South Africa”. The AstraZeneca ChAdOx1 vaccine results stated “All forty-two endpoint cases were graded either as mild (vaccinees=15; placebo-recipients=17) or moderate (vaccinees=4; placebo-recipients=6) with no cases of severe disease or hospitalisation in either arm” … “of which 39 (95.1%) were B.1.351“. While the AZ ability to prevent hospitalization is inconclusive, there were no cases of hospitalization. Since the mRNA vaccines first dose show similar or superior results to the AZ and Johnson vaccines, they could be expected to perform similarly or better against B.1.351.
It is important to realize that, while protection against current variants is desirable, it is perhaps even more desirable to prevent further variants. A 2x population vaccinated with dose 1 produces far fewer total viral replications than does a 1x population with 2 doses. Reducing total viral replications reduces opportunities for mutation / variants. The polyclonal immune response to viral exposure and/or vaccine reduces probability of infection from variants, or reduces infection severity and symptoms. Only dramatic variant mutations fully escape polyclonal immune response and result in a fully naive infection. “The isolation and characterization of 206 RBD-specific monoclonal antibodies derived from single B cells” has been performed. The remaining spike epitopes significantly add to this number of diverse clones. It is highly unlikely that a variant within the pandemic era would completely escape the full diversity of a prior immune response and develop into a serious case. That said, continuing study and vaccine development is prudent.
Preventing future variants is best achieved by minimizing total viral replications. A 2x population vaccinated with dose 1 produces far fewer total viral replications than does a 1x population with 2 doses.
Evidence For COVID-19 Vaccine Deferred Dose 2 Boost Timing also on OSF: https://doi.org/10.31219/osf.io/4p3bt
“We therefore provide real-world evidence for a high level of protection against asymptomatic SARS-CoV-2 infection after a single dose of BNT162b2 vaccine, at a time of predominant transmission of B.1.1.7 and … low frequency of prior infection (7.2% antibody positive).”
Rapid Dose Interval Likely Increases Unpleasant Side Effects Of Dose 2
Regarding vaccine side-effects, many have noted multiple days of quite encumbering symptoms associated with dose 2 when given at < 30 day intervals. Interestingly, IgM (and IgG) unbound antibody immune responses are generally peaking around the 15 to 30 day period past dose 1 vaccination. It is possible that the “warp speed” trial’s < 30 day dose 2 boost timing that was sharply designed to rapidly determine some understanding of vaccine efficacy, not as an optimal boost timing period, is contributing to these significant symptoms. A longer interval between doses would likely reduce these 2nd dose “side-effect” symptoms and improve long-term durability. Certain vaccines (e.g., adult tetanus and diphtheria toxoids [Td], pediatric diphtheria and tetanus toxoids [DT], tetanus toxoid) produce increased rates of local or systemic reactions in certain recipients when administered more frequently than recommended.
If I already had COVID-19, should I get a vaccine? “Our recommendation is to get the vaccine, because we don’t know how long natural immunity from being sick will last,” Tuznik said. “We also recommend waiting until 90 days after all symptoms have disappeared.” The reason for the wait: You will have some antibodies from the disease and are not likely to get COVID-19 again for at least 90 days, the CDC says. The waiting period will help reduce your reactions to the vaccine, plus it will let others who are more at risk get vaccinated first.
On June 23, 2021, ACIP met to review reported cases of myocarditis or pericarditis in mRNA COVID-19 vaccine (Pfizer-BioNTech and Moderna) recipients. Cases of myocarditis or pericarditis have occurred predominantly in males aged 12-29 years, with symptoms typically developing within a few days after receipt of the second dose of vaccine. – CDC 7/2/2021
While the vaccines have proven very favorable for reducing the impact of COVID-19 on many who are not in low-risk categories, improved research could lower the risk of the vaccine to those who are at very low risk of severe COVID-19.
“America First” Dose Interval Issues
As of 3/11/2021, the US Vaccination Program has not yet acknowledged the superior overall result of accelerating vaccinations by delaying dose 2 as the UK, Canada, and others have done. Canada has chosen a 4 month interval between doses so that many people may be rapidly vaccinated with dose 1. The current US interval of less than 30 days between doses is not only leaving US citizens unprotected, but is also doubling the near-term US demand for vaccine that could help other countries such as those in the EU which are scrambling to obtain vaccine that the US is hoarding. Italy has considered legal action against Pfizer because Pfizer is not meeting shipment commitments it made to Italy. Meanwhile, the US has over 29,000,000 doses in storage as of 3/9/2021 because of limitations of staff to perform vaccinations. Adding the 32,000,000 who have been doubly vaccinated to the 29,000,000 doses in storage leaves a total of 61 million additional Americans who could have been vaccinated with dose 1 as of 3/9/2021; but instead, they are unprotected. Or, the US could have shared some of those 61 million doses with other countries.

Clearly Defining Re-exposure Protection And Vaccine Efficacy Statistical Results
It is important to recognize that zero “serious” cases occurred in the vaccine arm of both Pfizer and Moderna Phase 3 trials after dose 1. There was 1 hospital visit associated with Pfizer that did not result in admission. An initially incorrectly classified case in the Moderna trial eventually was judged to have resulted in 1 hospitalization but was not categorized as “serious” by the NEJM article. The protection from “serious” cases (as stated by the trial publications) for both doses is virtually 100% and both of the hospital visits occurred after dose 2 and not in the period prior to dose 2. The vaccines have been shown to often result in side effects including fever, fatigue, myalgia, headaches, and other symptoms. If a single dose of vaccine prevents serious cases and death, and largely limits infection to non-pathologic symptoms, why would anyone care about efficacies that relate to preventing non-pathologic symptoms? If serious infection and death is prevented virtually 100% by a single dose, isn’t that enough to justify doubling the vaccinated population? And delaying the 2nd dose actually extends the long-term durability that dose 2 so aptly provides.

“There’s good reason to expect that the 12-week prime-boost interval recommended in the UK will lead to stronger, longer lasting immunity than the shorter doses recommended by the manufacturers.”


with those seen in the interim analysis of the trials and confirm that the vaccine
is efficacious, with results varying by dose interval in exploratory analyses. A 3-month
dose interval might have advantages over a …
“It has been suggested that an interval of at least 2-3 months between the prime and the boost is necessary to obtain optimal responses, as memory T cells with high proliferative potential do not form until several weeks after the first immunization, and memory 𝐵 cells have to go through the germinal center reaction and take several months to develop”
“The boost efficiency increases when the second dose is given 45 to 90 days after the prime”


Debunking Pfizer 52% Dose 1 Efficacy
The Phase 3 Trial 52.4% Pfizer dose 1 efficacy calculation, published in the NEJM on December 31 2020, was based on data starting the day that dose 1 was given, allowing zero time for it to take effect. It appears to be a mistake that’s hard to believe is even possible in an NEJM publication. Further, it’s amazing that the apparent mistake has not been publicly corrected by the NEJM as it continues to propagate in popular press articles and even other scientific publications. It is flat out befuddling that an apparent mistake like this remains so well concealed among popular press and the general public while being so widely acknowledged as a “miscommunication” throughout the scientific community.
Read Evidence For COVID-19 Vaccine Deferred Dose 2 Boost Timing
Regarding dose 1 “Using data for those cases observed between day 15 and 21, efficacy against symptomatic COVID-19 was estimated at 89%” – UK Department of Health & Social Care
Read Stanley Plotkin and Neal Halsey’s article.
Also listen to the Wachter interview (below) at minute 11:00 for info on the 52% “miscommunication”.
Also listen to similar in Wachter / Offit JAMA interview.
Also listen to Marty Makary interview.
Also read the Letter to the Editor published by the NEJM on February 17, 2021
Dose 2 is important for long-term durability, and delayed dose 2 timing helps – see above.



On Feb 17, 2021, the NEJM published a Letter to the Editor that stated: “Even before the second dose, BNT162b2 was highly efficacious, with a vaccine efficacy of 92.6%, a finding similar to the first-dose efficacy of 92.1% reported for the mRNA-1273 vaccine (Moderna).“. It would be prudent for the NEJM to resolve the ambiguity between the 52.4% dose 1 efficacy in the original NEJM published article, and this NEJM published Letter to the Editor stating dose 1 efficacy of 92.6%. The NEJM should clearly state that the 52.4% dose 1 efficacy calculation was based on an invalid efficacy calculation method that was different from the valid method used to calculate dose 2 and that the dose 1 efficacy is in the range of 82% to 93% depending upon calculation methods, and reference Evidence For COVID-19 Vaccine Deferred Dose 2 Boost Timing which stated this on Jan 5. 2021.

Medical Expert Interviews

A question of legal implications of “someone receiving dose 1 that died because they didn’t get dose 2 in a timely manner” also begs the question: “what if someone who doesn’t get dose 1 dies because someone else was prioritized to receive 2 doses before the other person received dose 1”? It is quite clear from the trial data that the latter of these 2 scenarios is far more likely as there were zero hospital admissions in the vaccine arm after dose 1. In fact, while the evidence of zero hospitalizations might produce 1 odd case of the former, the latter would likely be a class action with size in the 10’s of thousands.
Another question of messaging was raised about dose 2 timing alteration possibly creating public confusion. First, there is an app that reminds people of when to get dose 2. That can easily be adjusted. When the Space Shuttle Challenger exploded, many engineers and low level manager were trying to convince launch officials of safety issues – seven crew died because the data was ignored. Data shows that deferring dose 2 will save many 10K’s of US lives. Not disclosing this data to the public and allowing 10K’s of people to die and larger volumes to be hospitalized and passing it off as a messaging problem is tantamount to deception and possibly even criminal. To eliminate public confusion, this web page exists to clarify numerous areas of miscommunication and obfuscation. As part of dose 2 timing optimization, dose 1 could be given and monitored and then dose 2 timing adjusted based on real-time data. A good starting point for dose 2 timing is anywhere in the 3 to 5 month range as stated in the article at the top of this page. If a call is made to adjust it based on real-time data, the public could feel secure that it is being optimized based on real-time data within that range. Or, pick a number within that range and stick with it. Anything that allows lives to be saved by delaying dose 2 is a welcome, intelligent choice. Please read everything on this page to understand the reasons for this approach. This is a public page and anyone can read it and research further, providing public, transparent, and detailed understandings about dose 2 timing. A license to copy this page’s content is hereby granted to the US Federal government, as long as a link to this page and a citation is included at a visible location at the top of the copied content. We’re here to help save lives. communicate, and educate.

“Although we understand the argument for sticking with the original vaccine schedule, we worry that analysts have concentrated on the risks of deviating from the prescribed schedule while ignoring the risks of adhering to it.” … “An evaluation from Brazil showed that the Chinese Sinovac Biotech vaccine was 20% more effective in a sub-group of patients who waited longer for their booster dose.” … “We need to balance the risk of prolonging the interval between doses against the risk of vaccinating only half as many people in the near term, which could result in an additional 480,000 hospitalizations and 54,000 deaths.” – Michael H Criqui, MD, MPH is a Distinguished Professor at the University of California, San Diego School of Medicine, past Chief of the Division of Preventive Medicine, epidemiologist, Preventive Medicine specialist, Robert M. Kaplan, UCLA distinguished research professor of health policy and management and medicine, adjunct professor of medicine at Stanford University, Past chief science officer at the US Agency for Health Care Research and Quality (AHRQ) and associate director of the National Institutes of Health
In a most perplexing move, the FDA is signaling that changing the RNA in the mRNA vaccines will not require large clinical trials, yet the same FDA is hesitant to adopt delayed dose 2 timing.
http://www.crchudequebec.ulaval.ca/en/research/researchers/gaston-de-serres/
Remember when the WHO said: “There is currently no evidence that people who have recovered from COVID-19 and have antibodies are protected from a second infection”? That was an error. Even at that time, immunological evidence to the contrary did exist.
Remember back in March-April 2020 when the protocol was immediate intubation? That was an error.
And so is using the non-optimal accelerated dose schedule used during the rapid efficacy trials that was helpful for getting rapid data on efficacy and safety. Read the rest in manuscript above.
Currently, a partial list of experts that suggest benefits and/or lack of negative consequences for delaying dose 2 includes: Marty Makary, Zubin Damania, Christopher J. Gill, Wes Ely, Soren Brostrom, Donald Vinh, Richard Massé, Theresa Tam, Danuta Skowronski, Gaston De Serres, Leif-Erik Sander, Michael Criqui, Robert M. Kaplan, Buddy Creech, Paul Sax, Robert Wachter, Ashish K. Jha, David Salisbury, Chris Whitty, Michael Osterholm, Zeke Emanuel, Stanley A. Plotkin, Neal Halsey. Please contact Really Correct with others that should be considered for inclusion in this life-saving list.
Please also see Immunology: Vaccines, Viral Loads, Symptom Severity, And Immunity
On an individual basis, follow the direction of your personal physician. This information is aimed at improving US epidemiologic response.